
Investigações
Primeiras investigações a serem solicitadas
radiografia torácica
Exame
Em pacientes hospitalizados, geralmente é necessário apresentar evidências radiológicas de nova condensação em radiografia torácica para confirmar o diagnóstico de PAC.[74][77][89]
Realizar radiografia torácica em todos os pacientes que chegarem ao hospital com suspeita de pneumonia adquirida na comunidade (PAC) dentro de 4 horasapós a admissão.[78][Figure caption and citation for the preceding image starts]: Radiografia de tórax posteroanterior mostrando consolidação do lobo superior direito em um paciente com pneumonia adquirida na comunidadeDurrington HJ, et al. Recent changes in the management of community acquired pneumonia in adults. BMJ 2008;336:1429. [Citation ends].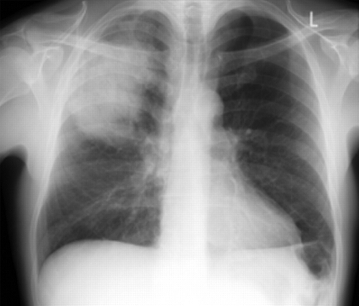 [Figure caption and citation for the preceding image starts]: Radiografia de tórax mostrando pneumonia cavitando no lobo superior esquerdoDa coleção do Dr. Jonathan Bennett. Usado com permissão [Citation ends].
[Figure caption and citation for the preceding image starts]: Radiografia de tórax mostrando pneumonia cavitando no lobo superior esquerdoDa coleção do Dr. Jonathan Bennett. Usado com permissão [Citation ends]. [Figure caption and citation for the preceding image starts]: Derrame pleural no lado esquerdoDa coleção do Dr. R Light. Usado com permissão [Citation ends].
[Figure caption and citation for the preceding image starts]: Derrame pleural no lado esquerdoDa coleção do Dr. R Light. Usado com permissão [Citation ends]. [Figure caption and citation for the preceding image starts]: Opacificação aumentada da região peri-hilar direita e do segmento superior dos lobos inferior e superior direitos, compatível com agravamento da pneumonia por aspiraçãoDa coleção do Dr. Roy Hammond. Usado com permissão [Citation ends].
[Figure caption and citation for the preceding image starts]: Opacificação aumentada da região peri-hilar direita e do segmento superior dos lobos inferior e superior direitos, compatível com agravamento da pneumonia por aspiraçãoDa coleção do Dr. Roy Hammond. Usado com permissão [Citation ends].
Se a radiografia torácica mostrar alterações atípicas ou pneumonia complicada (por exemplo, cavitação, derrame pleural, consolidação multifocal), considere outros exames de imagem (consulte Outros exames a serem considerados).
Practical tip
Uma radiografia de boa qualidade é muito importante para um diagnóstico preciso e para evitar a prescrição inadequada de antibióticos. Um estudo relatou que 29% dos pacientes hospitalizados tratados para PAC não apresentaram anormalidades radiográficas.[102]
Pode ser mais difícil obter uma radiografia torácica de qualidade adequada em pessoas com obesidade grau III (IMC ≥40 kg/m²).
Nãosolicite rotineiramente uma radiografia torácica em pacientes com suspeita de PAC atendidos na comunidade, a menos que:[74][77]
Haja dúvida diagnóstica
na avaliação, a evolução clínica após o tratamento não foi satisfatória
o paciente apresenta fatores de risco para patologias pulmonares subjacentes, como câncer pulmonar.
Resultado
novo sombreamento (consolidação)
oximetria de pulso
Exame
Utilize a oximetria de pulso (de preferência em ar ambiente) para avaliar a saturação de oxigênio tanto em ambientes hospitalares quanto em unidades de atenção primária.[74][77][84] Isso ajuda a orientar o tratamento de suporte imediato e a avaliar a gravidade da situação.[84]
Resultado
pode revelar baixa saturação de oxigênio
gasometria arterial
Exame
Realizar gasometria arterial em pacientes hospitalizados com PAC que apresentem:[84]
SpO₂ <94% em ar ambiente ou necessidade de oxigênio suplementar para manter a saturação alvo
necessidades elevadas de oxigênioouaumento da FiO₂
fatores de risco para hipercapnia (por exemplo, DPOC, síndrome da hipoventilação-obesidade, distúrbios neuromusculares ou deformidade da parede torácica), especialmente com torpor ou agravamento da dispneia
doença de alta gravidade ou doença crítica (consulte os critérios de diagnóstico para obter orientações sobre a avaliação da gravidade)
deterioração clínica , incluindo:
dispneia em agravamento
queda na saturação de oxigênio (≥3%)
aumento do NEWS2 ou de outros indicadores de alerta precoce
suspeita de distúrbio metabólico (por exemplo, cetoacidose diabética ou insuficiência renal)
qualquer situação em que os resultados da gasometria arterial possam informar o manejo.
Practical tip
A obtenção de uma gasometria enquanto o paciente ainda não está recebendo oxigênio suplementar fornece uma avaliação mais acurada do estado de oxigenação, mas não deve atrasar a administração de oxigênio suplementar em um paciente instável.
Registre sempre a fração de oxigênio inspirado (FiO₂) de forma clara, pois isso é essencial para a interpretação dos resultados da gasometria arterial.
Para avaliação inicial, pode-se utilizar uma gasometria venosa, especialmente quando uma gasometria arterial não for imediatamente indicada. Pode apresentar alcalose respiratória, acidose metabólica (por exemplo, devido à hipotensão, perfusão tecidual reduzida ou lesão renal aguda) ou lactato elevado. No entanto, a gasometria venosa não avalia a oxigenação de forma confiável e pode não refletir com precisão os níveis de dióxido de carbono arterial; se as necessidades de oxigênio forem elevadas ou se a gasometria venosa sugerir possível acidose respiratória, realize uma gasometria arterial para avaliar a oxigenação e a ventilação.[84]
Como alternativa à amostragem arterial, a gasometria de sangue arterializado do lóbulo da orelha (capilar) pode ser utilizada para obter uma medida precisa do pH e da PaCO₂. No entanto, a PaO₂ é menos precisa (normalmente subestimada em 0.5-1.0 kPa), portanto, a saturação de oxigênio deve ser monitorada cuidadosamente e uma gasometria arterial deve ser realizada caso haja alguma preocupação com a precisão.[84]
Resultado
pode apresentar hipoxemia ou hipercapnia
pode revelar acidemia (respiratória ou metabólica)
pode revelar lactato elevado, potencialmente indicando sepse
ureia e eletrólitos
Exame
Solicite dosagem de ureia e eletrólitos em pacientes sendo investigados no hospital para dar suporte à avaliação da gravidade eavaliar a função renal.[74][77]
A doença renal crônica é um fator de risco significativo para mortalidade nos pacientes com PAC.[69]
Exames de sangue de rotina, incluindo ureia e eletrólitos, não são necessários para a maioria dos pacientes acompanhados na comunidade, mas devem ser realizados em todos os pacientes hospitalizados.[74][77]
Resultado
geralmente normal; a ureia pode estar elevada em pacientes com PAC grave
ureia >7 mmol/L (>19.6 mg/dL) corresponde a 1 ponto no escore CURB-65 para avaliação do risco de mortalidade
lesão renal aguda pode ocorrer em pacientes com sepse que complica a PAC
hemograma completo
Exame
A leucocitose é frequentemente observada em pessoas com PAC.
Exames de sangue de rotina, incluindo hemograma completo, não são necessários para a maioria dos pacientes acompanhados na comunidade, mas devem ser realizados em todos os pacientes hospitalizados.[74][77]
Resultado
leucocitose é comum
Uma contagem leucocitária >15 × 109/L sugere infecção bacteriana (particularmente pneumocócica), embora contagens mais baixas não descartem uma causa bacteriana
proteína C-reativa
Exame
Solicitar proteína C-reativa em pacientes internados para investigação, a fim de auxiliar no diagnóstico e fornecer uma medida basal.[74]
Níveis elevados de proteína C-reativa não distinguem de forma confiável a PAC bacteriana da não bacteriana; no entanto, níveis baixos de proteína C-reativa tornam a etiologia bacteriana menos provável.[118]
O National Institute for Health and Care Excellence (NICE) do Reino Unido também recomenda considerar a medição da proteína C-reativa (ou procalcitonina) 3-4 dias após o início do tratamento, caso haja preocupação clínica com a falha do tratamento.[78]
Níveis elevados de proteína C-reativa, ou níveis que não melhoram significativamente com o tratamento, estão associados à falha do tratamento e podem indicar a necessidade de avaliação clínica por um profissional mais experiente.[78]
Uma falha em reduzir a proteína C-reativa em ≥50% até o 4º dia está associada a maior mortalidade em 30 dias, maior necessidade de ventilação mecânica e maior probabilidade de outras complicações.[119]
Exames de sangue de rotina, incluindo a proteína C-reativa, não são necessários para a maioria dos pacientes acompanhados na comunidade, mas devem ser realizados em todos os pacientes hospitalizados.[74][77]
Resultado
elevada
Proteína C-reativa >100 mg/L corrobora o diagnóstico de pneumonia
Proteína C-reativa <20 mg/L (em um paciente com sintomas há >24 horas) tornam a pneumonia improvável
testes da função hepática
Exame
Obtenha testes da função hepática (TFHs) basais em todos os pacientes hospitalizados.[74][77]
Os resultados geralmente são normais, mas podem ser anormais em pessoas com doença hepática subjacente ou infecção por Legionella pneumophila.[74]
A doença hepática crônica é um fator de risco para complicações pulmonares em pacientes hospitalizados devido à pneumonia pneumocócica.[71]
Exames de sangue de rotina, incluindo TFHs, não são necessários para a maioria dos pacientes acompanhados na comunidade, mas devem ser realizados em todos os pacientes hospitalizados.[74][77]
Resultado
geralmente normal; pode ser anormal em pacientes com doença hepática subjacente ou infecção por Legionella pneumophila
Investigações a serem consideradas
hemocultura
Exame
No ambiente hospitalar, considere a realização de hemoculturas em pacientes com pneumonia adquirida na comunidade (PAC) de gravidade moderada ou alta (conforme determinado pelo escore CURB-65 e julgamento clínico, consulte Critérios de diagnóstico) se houver indicações clínicas adicionais, como suspeita de sepse.[78]
Idealmente, as hemoculturas devem ser coletadas antes do início da antibioticoterapia, pois a antibioticoterapia prévia pode reduzir a quantidade de culturas positivas e afetar os resultados.[78]
O isolamento de bactérias pode ser altamente específico na determinação da etiologia microbiana em pessoas com PAC de gravidade moderada ou alta.[74][77]
A bacteriemia também é um marcador da gravidade da doença. No entanto, muitos pacientes com PAC não têm bacteremia associada.[74]
As causas microbianas da PAC que podem ser associadas à bacteremia incluem:[74][120]
Streptococcus pneumoniae (identificado em aproximadamente 60% das hemoculturas positivas)
Haemophilus influenzae (identificado em 2% a 13% das culturas positivas)
Staphylococcus aureus e Klebsiella pneumoniae
Não solicite exames microbiológicos, incluindo hemoculturas, de rotina em pacientes com PAC de baixa gravidade ou em pacientes com PAC que estejam sendo tratados na comunidade.[78][74][77]
Resultado
crescimento do patógeno bacteriano causador
cultura de escarro
Exame
no hospital
Considere a cultura de escarro em:
Todos os pacientes com PAC de gravidade moderada ou alta (conforme determinado pelo escore CURB-65 e avaliação clínica - consulte os critérios de diagnóstico), levando em consideração a história de tratamento com antibióticos, a evolução clínica, a presença de comorbidades, qualquer hospitalização recente e a probabilidade de obtenção de uma amostra de escarro de boa qualidade.[74][77][78]
Pacientes que não apresentarem melhora com a terapia inicial, independentemente da gravidade da doença.[74][77]
Não solicite exames microbiológicos, incluindo cultura de escarro, de rotina em pacientes com PAC de baixa gravidade.[78]
Na comunidade
Não solicite exames microbiológicos de rotina, incluindo cultura de escarro, em pacientes com PAC que estejam sendo tratados na comunidade.[74][77]
Considere solicitar exames microbiológicos na comunidade somente se:[74]
Os sintomas do paciente não melhoram com a antibioticoterapia empírica
O paciente apresenta tosse produtiva persistente, especialmente se também apresentar mal-estar, perda de peso ou sudorese noturna, ou fatores de risco para tuberculose (por exemplo, origem étnica, privação social, idade avançada, história pregressa de tuberculose, história de contato com tuberculose): considere a realização de exame de escarro para Mycobacterium tuberculosis.
Há uma razão clínica ou epidemiológica, como um surto(por exemplo, doença do legionário) ou durante epidemias de micoplasma: considere o teste de antígeno urinário, reação em cadeia da polimerase de amostras do trato respiratório superior (por exemplo, swabs nasais e de garganta) ou inferior (por exemplo, escarro) ou investigações sorológicas; se disponível, a reação em cadeia da polimerase é preferível às investigações sorológicas.
Resultado
crescimento do patógeno bacteriano causador
teste de antígeno urinário para Streptococcus pneumoniae
Exame
no hospital
Considere a realização de teste de antígeno urinário pneumocócico (detecta S pneumoniae) em pessoas com PAC de gravidade moderada ou alta.[78]
O teste de antígeno urinário é útil para o diagnóstico de pneumonia pneumocócica em adultos e é menos afetado por antibioticoterapia prévia do que as culturas de sangue/escarro.[74][77]
Não solicite rotineiramente exames microbiológicos, incluindo testes de antígeno urinário, em pacientes com PAC de baixa gravidade que chegam ao hospital.[78]
Na comunidade
Não solicite exames microbiológicos de rotina, incluindo testes de antígeno urinário, em pacientes com PAC que estejam sendo tratados na comunidade.[74][77]
Evidência: Teste de antígeno urinário para pneumonia pneumocócica
Estudos demonstraram que o teste de antígeno urinário para pneumococos tem uma sensibilidade significativamente maior que as culturas de sangue ou de escarro de rotina.[121]
Os resultados permanecem positivos em 80% a 90% dos pacientes por até 7 dias após o início do tratamento antimicrobiano.[121]
Resultado
pode ser positiva
teste de antígeno urinário para Legionella pneumophila
Exame
no hospital
O National Institute for Health and Care Excellence (NICE) recomenda considerar o teste de antígeno urinário para legionella em pacientes que chegam ao hospital com PAC de gravidade moderada ou alta e que apresentam fatores de risco específicospara infecção por legionella.[78]
Os fatores de risco epidemiológicos incluem:[45][131]
Viagens recentes, especialmente com pernoites fora de casa (incluindo hotéis ou navios de cruzeiro)
Exposição a sistemas de água potencialmente contaminados (por exemplo, banheiras de hidromassagem, piscinas de spa ou sistemas de encanamento complexos)
Atendimento recente em uma unidade de saúde
Utilização de equipamentos de terapia respiratória
Associação com um surto conhecido ou suspeito de legionela
Além disso, os seguintes grupos de pacientes têm um maior risco de infecção por Legionella:[131][132]
Idade >50 anos
Sexo masculino
Tabagismo (presente ou anterior)
Doença pulmonar crônica (como DPOC ou enfisema)
Comorbidades subjacentes, incluindo cardiopatia, diabetes, insuficiência renal ou insuficiência hepática
Malignidade sistêmica
Imunocomprometimento devido a doença ou a medicamentos imunossupressores
O diagnóstico precoce da pneumonia por legionella é importante porque está associada a uma mortalidade significativa e tem implicações para a saúde pública.[74][77]
O ensaio imunoenzimático para antígeno urinário proporciona detecção rápida, altamente específica (>95%) e moderadamente sensível (80%) de L pneumophila sorogrupo 1, a principal causa de PAC associada à legionela no Reino Unido.[74][124][77]
Para todos os pacientes que apresentarem resultado positivo para o antígeno urinário de Legionella, uma amostra do trato respiratório inferior (por exemplo, escarro, lavagem broncoalveolar ou tecido pulmonar post-mortem) deve ser obtida o mais breve possível e testada para espécies de Legionella por reação em cadeia da polimerase e cultura.[74][77][132]
O NICE recomenda que não se solicitem rotineiramente exames microbiológicos, incluindo testes de antígeno urinário, em pacientes com PAC de baixa gravidade.[78] No entanto, a British Thoracic Society (BTS) recomenda que o teste de antígeno urinário para L pneumophila seja considerado em pacientes com PAC de baixa gravidade nas seguintes situações:[74]
Durante surtos
Quando houver uma razão clínica ou epidemiológica específica
Na comunidade
Não solicite exames microbiológicos de rotina, incluindo testes de antígeno urinário, em pacientes com PAC que estejam sendo tratados na comunidade.[74][77] De acordo com a BTS, o teste de antígeno urinário para legionela pode ser considerado em circunstâncias selecionadas, quando houver uma indicação clínica ou epidemiológica específica, como durante surtos (por exemplo, doença do legionário) ou quando a exposição epidemiológica relevante levantar suspeita de infecção por legionela.[74][77]
Resultado
pode ser positiva
reação em cadeia da polimerase e/ou testes sorológicos
Exame
A reação em cadeia da polimerase pode auxiliar na identificação rápida do patógeno causador. A British Thoracic Society (BTS) não recomenda a realização de testes de reação em cadeia da polimerase como rotina para todos os pacientes com PAC. Em vez disso, a reação em cadeia da polimerase é posicionada como uma ferramenta diagnóstica direcionada para ser usada em circunstâncias clínicas selecionadas, particularmente onde a identificação de patógenos virais ou atípicos puder influenciar o tratamento.[74][77]
Em pacientes com PAC de alta gravidade, a BTS recomenda que testes de reação em cadeia da polimerase em amostras do trato respiratório (por exemplo, escarro ou swab do trato respiratório superior) podem ser considerados para permitir a identificação rápida de vírus respiratórios e patógenos atípicos, particularmente quando:[74][77]
houver uma resposta inadequada à antibioticoterapia inicial e/ou
existe forte suspeita clínica de causa viral ou atípica da pneumonia.
Os patógenos de interesse incluem vírus respiratórios (por exemplo, influenza A e B, parainfluenza 1-3, adenovírus, vírus sincicial respiratório) e bactérias atípicas (por exemplo, Mycoplasma pneumoniae, Chlamydia pneumoniae, Chlamydia psittaci, Coxiella burnetii e Pneumocystis jirovecii).[74][77]
Em pacientes com PAC de gravidade leve ou moderada, a BTS recomenda que o teste de reação em cadeia da polimerase não seja realizado rotineiramente. A reação em cadeia da polimerase pode ser considerada apenas em circunstâncias selecionadas, incluindo:[74]
Surtos
Anos epidêmicos para patógenos específicos (por exemplo, M pneumoniae)
Quando houver uma indicação clínica ou epidemiológica específica que levante a suspeita de um patógeno atípico ou viral
Nas diretrizes da BTS para PAC, os testes sorológicos referem-se a exames de sangue baseados em anticorpos utilizados para detectar infecções por patógenos respiratórios atípicos (por exemplo, M pneumoniae, espécies de Chlamydia, C burnetii). A BTS nãorecomenda a sorologia para o diagnóstico de rotina da PAC devido ao seu valor limitado no manejo do quadro agudo e afirma que a reação em cadeia da polimerase é preferível quando disponível, pois fornece resultados mais precoces e clinicamente mais úteis.[74] No entanto, observa-se que os testes sorológicos podem ser considerados em circunstâncias específicas, incluindo:[74][77]
quando os testes de reação em cadeia da polimerase não estão disponíveis, particularmente para patógenos atípicos suspeitos,
em pacientes com PAC de alta gravidade, nos quais nenhum diagnóstico microbiológico foi feito por outros métodos e o paciente não apresenta melhora,
durante surtos ou períodos epidêmicos, quando a confirmação do organismo causador é importante para a vigilância em saúde pública, e
para diagnóstico retrospectivo, investigação epidemiológica ou auditoria, e não para orientar a terapia inicial.
Nesses contextos, a sorologia pareada (amostras da fase aguda e da fase de convalescência) é preferível à titulação única, pois melhora a confiabilidade diagnóstica.[74]
Resultado
detecção de antígenos ou anticorpos patogênicos virais/atípicos
Teste para SARS-CoV-2 (reação em cadeia da polimerase ou antígeno)
Exame
Considere a realização do teste para SARS-CoV-2 se houver suspeita clínica de COVID-19 e o resultado puder influenciar o tratamento. Consulte Doença do coronavírus de 2019 (COVID-19).[90]
Resultado
positivo em pacientes com infecção por COVID-19
TC do tórax
Exame
Considere a realização de uma TC do tórax quando houver dúvidas diagnósticas (por exemplo, se a radiografia torácica for de má qualidade ou mostrar consolidação mal definida) ou quando houver achados complexos ou atípicos na radiografia torácica, tais como:[74][111]
Cavitação: a TC pode ajudar a identificar diagnósticos alternativos, como tuberculose, câncer pulmonar, infarto pulmonar, embolia pulmonar séptica, bolha infectada ou abscesso pulmonar.
[Figure caption and citation for the preceding image starts]: Radiografia de tórax mostrando pneumonia cavitando no lobo superior esquerdoDa coleção do Dr. Jonathan Bennett. Usado com permissão [Citation ends].
Consolidação multifocal: a TC pode ajudar a identificar diagnósticos alternativos, como infecção estafilocócica, tuberculose, pneumonia por aspiração, aspergilose broncopulmonar alérgica, pneumonia em organização criptogênica ou pneumonite induzida por medicamentos.
Derrame pleural: a TC (em conjunto com ultrassonografia torácica e aspiração guiada) pode ajudar a identificar derrames parapneumônicos, empiema, tuberculose, câncer pulmonar ou derrames reativos/inflamatórios.
Aproximadamente 20% a 57% dos pacientes hospitalizados com pneumonia desenvolvem derrame parapneumônico.[112]
[Figure caption and citation for the preceding image starts]: Derrame pleural no lado esquerdoDa coleção do Dr. R Light. Usado com permissão [Citation ends].
Resultado
pode apresentar cavitação, derrame pleural, consolidação multifocal ou uma neoplasia subjacente
ultrassonografia do pulmão
Exame
Dependendo da disponibilidade, a ultrassonografia pulmonar pode representar uma técnica prática e acessível para o diagnóstico de PAC. Ela é um método de imagem livre de radiação e uma alternativa útil quando o médico possui treinamento e equipamentos adequados. A ultrassonografia pulmonar é particularmente valiosa quando a radiografia torácica não está disponível.
Evidências: Ultrassonografia no diagnóstico de PAC
Evidências mostram que a ultrassonografia pulmonar pode diagnosticar a pneumonia em adultos com excelente acurácia, inclusive no pronto-socorro.[103][104][105] Uma metanálise que utilizou a TC como padrão de referência constatou que a ultrassonografia foi mais precisa do que a radiografia torácica para o diagnóstico de PAC.[106]
No Reino Unido, o National Institute for Health and Care Excellence (NICE) recomenda que a ultrassonografia pulmonar seja um recurso útil no diagnóstico de PAC em situações específicas, incluindo:[78]
Avaliação rápida no local de atendimento de um paciente doente ou em deterioração
Avaliação de possíveis diagnósticos alternativos, como insuficiência cardíaca
Investigação de complicações, incluindo derrame pleural ou outras doenças da pleura
[Figure caption and citation for the preceding image starts]: Derrame pleural no lado esquerdoDa coleção do Dr. R Light. Usado com permissão [Citation ends].
Recomendações semelhantes são refletidas nas diretrizes dos EUA:
A American Thoracic Society afirma que, para adultos com suspeita de PAC, a ultrassonografia pulmonar é uma alternativa diagnóstica aceitável à radiografia torácica em centros médicos onde haja experiência clínica adequada.[107]
O American College of Physicians recomenda a ultrassonografia no local de atendimento (POCUS) nos casos de incerteza diagnóstica em pacientes que se apresentarem com dispneia aguda.[108]
O American College of Radiology observa que a POCUS é particularmente útil quando o acesso à TC é limitado, como quando é necessária uma avaliação rápida ou quando a condição do paciente limita sua mobilidade ou o transporte até a sala de radiologia.[109]
Practical tip
O diagnóstico de PAC por meio de ultrassonografia pulmonar à beira do leito depende principalmente da detecção de condensação. No entanto, a condensação nem sempre está presente, pois a pneumonia pode ser intersticial ou manifestar-se como infiltrados pulmonares difusos. Nesses casos, correlacione com os achados clínicos e considere exames de imagem alternativos se a incerteza diagnóstica persistir.
Resultado
consolidação pode ser observada; derrame parapneumônico pode ser visto
toracocentese e cultura do líquido pleural
Exame
Realize toracocentese diagnóstica precoce em todos os pacientes com derrame pleural para avaliar a presença de infecção no espaço pleural devido a derrame parapneumônico complicado (derrame parapneumônico que requer drenagem, mesmo que não seja francamente purulento) ou empiema.[74][77]
A presença de pus, líquido turvo ou organismos na coloração de Gram ou na cultura é diagnóstica de empiema.
Líquido pleural não purulento com pH <7.2 no contexto de PAC é compatível com derrame parapneumônico complicado, sugerindo invasão bacteriana do espaço pleural.
Drene o líquido pleural nos pacientes com empiema confirmado ou líquido pleural não purulento com pH <7.2.[74]
Resultado
empiema: pus; líquido pleural turvo; microrganismos visíveis na coloração de Gram ou em cultura
derrame parapneumônico complicado: pH do líquido pleural <7.2 no contexto de PAC
angiografia pulmonar por tomografia computadorizada (APTC)
Exame
Considere a realização de uma APTC para avaliar a possibilidade de embolia pulmonar se os sintomas surgirem rapidamente (em minutos) ou se a dor torácica e a dispneia precederem os sintomas infecciosos.[113]
A APTC apresenta a maior acurácia diagnóstica entre as modalidades de imagem não invasivas para embolia pulmonar.[114]
Resultado
pode apresentar uma falha de enchimento intraluminal parcial ou completo dentro de uma artéria pulmonar, compatível com tromboembolismo.
broncoscopia
Exame
As diretrizes da British Thoracic Society recomendam considerar a broncoscopia em pacientes com sinais, sintomas e anormalidades radiológicas persistentes aproximadamente 6 semanas após a conclusão do tratamento.[74][77]
Resultado
secreções mucopurulentas; inflamação endobrônquica; obstrução por muco; patologias alternativas, incluindo neoplasia maligna, patógenos atípicos ou resistentes (incluindo tuberculose), bronquiectasia
procalcitonina sérica
Exame
O National Institute for Health and Care Excellence (NICE) do Reino Unido recomenda considerar a medição da procalcitonina (ou proteína C-reativa) 3 a 4 dias após o início do tratamento, caso haja preocupação clínica com a falha do tratamento.[78]
A procalcitonina é um peptídeo precursor da calcitonina, responsável pela homeostase do cálcio.
Concentrações elevadas de procalcitonina estão associadas à pneumonia bacteriana, enquanto concentrações mais baixas são mais comuns em pneumonias virais e atípicas. A procalcitonina apresenta níveis particularmente elevados em casos de pneumonia pneumocócica.[127][128]
Resultado
pode estar elevada na pneumonia bacteriana, particularmente na pneumonia pneumocócica
O uso deste conteúdo está sujeito ao nosso aviso legal