Hantavirus cardiopulmonary syndrome (HCPS) is a notifiable condition. Symptoms of early infection are nonspecific and can resemble many other febrile and respiratory illnesses. Therefore, early diagnosis is difficult. A history of peridomestic exposure to rodents or cleaning rodent-infested enclosures is an epidemiologic clue to diagnosing hantavirus infection. Contact with a known case of Andes virus (ANDV) infection during an outbreak is also relevant as human-to-human transmission has been reported with this species. It is important to consider hantavirus infection early in the differential diagnosis for patients with a relevant epidemiologic history. Serologic or molecular testing is required to confirm the diagnosis.
Infection prevention and control (IPC)
Standard precautions are recommended when managing all patients with hantavirus infection.[55]Centers for Disease Control and Prevention. Appendix A: type and duration of precautions recommended for selected infections and conditions. Feb 2025 [internet publication].
https://www.cdc.gov/infection-control/hcp/isolation-precautions/appendix-a-type-duration.html#H
[56]World Health Organization. Standard precautions for the prevention and control of infections: aide-memoire. Jun 2022 [internet publication].
https://www.who.int/publications/i/item/WHO-UHL-IHS-IPC-2022.1
Human-to-human transmission has been reported rarely with ANDV. If ANDV infection is suspected or confirmed, the patient should be placed in an isolation room, and contact and airborne precautions are recommended including use of a gown, eye protection, and a N95 (or higher-level) respirator when entering the patient’s room. Duration of precautions should be determined on a case-by-case basis in conjunction with local public health authorities.[6]Centers for Disease Control and Prevention. 2026 multi-country hantavirus cluster linked to cruise ship. May 2026 [internet publication].
https://www.cdc.gov/han/php/notices/han00528.html
[57]UK Health Security Agency. Andes hantavirus: epidemiology, outbreaks and guidance. Jun 2026 [internet publication].
https://www.gov.uk/guidance/andes-hantavirus-epidemiology-outbreaks-and-guidance
Stages of illness
HCPS infection is best understood as occurring in stages.[58]Mertz GJ, Hjelle B, Crowley M, et al. Diagnosis and treatment of new world hantavirus infections. Curr Opin Infect Dis. 2006 Oct;19(5):437-42.
http://www.ncbi.nlm.nih.gov/pubmed/16940866?tool=bestpractice.com
Following virus exposure there is an asymptomatic incubation period. A prodromal nonspecific viral illness follows with fever, headache, myalgias, and often prominent gastrointestinal (GI) symptoms.
During an early pulmonary syndrome phase there is increasing dyspnea and hypoxemia.
In the cardiopulmonary phase the patient is gravely ill with pulmonary edema, thrombocytopenia, hemoconcentration, and cardiogenic shock.
In those survivors of the cardiopulmonary phase, there follows a diuresis phase with resolution of the pulmonary edema. Convalescence may be prolonged.
Clinical presentation
Prodromal illness
Diagnosis is rarely made at this stage of illness due to nonspecific symptoms. Prodromal viral illness symptoms including fever, headache, myalgia, and GI symptoms (e.g., anorexia, nausea, vomiting, diarrhea, abdominal pain) are usually present.[5]Chapman LE, Ellis BA, Koster FT, et al. Discriminators between hantavirus-infected and -uninfected persons enrolled in a trial of intravenous ribavirin for presumptive hantavirus pulmonary syndrome. Clin Infect Dis. 2002 Feb 1;34(3):293-304.
http://cid.oxfordjournals.org/content/34/3/293.long
http://www.ncbi.nlm.nih.gov/pubmed/11774075?tool=bestpractice.com
Upper respiratory tract symptoms (e.g., sore throat, nasal congestion, sneezing), are rarely described with hantavirus infection and would tend to exclude the diagnosis.[5]Chapman LE, Ellis BA, Koster FT, et al. Discriminators between hantavirus-infected and -uninfected persons enrolled in a trial of intravenous ribavirin for presumptive hantavirus pulmonary syndrome. Clin Infect Dis. 2002 Feb 1;34(3):293-304.
http://cid.oxfordjournals.org/content/34/3/293.long
http://www.ncbi.nlm.nih.gov/pubmed/11774075?tool=bestpractice.com
Clinically, the patient may be tachypneic, but oxygen saturations will be normal.
Early pulmonary phase
Cardiopulmonary phase
Progression of the disease results in hypotension and pulmonary edema.
Patients may have dyspnea, chest tightness, and a cough as the lungs fill with fluid.[6]Centers for Disease Control and Prevention. 2026 multi-country hantavirus cluster linked to cruise ship. May 2026 [internet publication].
https://www.cdc.gov/han/php/notices/han00528.html
Late symptoms generally appear approximately 4 to 10 days after the initial phase of illness, with rapid deterioration over 24 hours. The critical phase is usually short.[6]Centers for Disease Control and Prevention. 2026 multi-country hantavirus cluster linked to cruise ship. May 2026 [internet publication].
https://www.cdc.gov/han/php/notices/han00528.html
Diuresis phase
The incubation period is typically 9 to 33 days (median 14-17 days, and up to 3 weeks after rodent bite).[35]Fritz CL, Young JC. Estimated incubation period for hantavirus pulmonary syndrome. Am J Trop Med Hyg. 2001 Nov;65(5):403.
http://www.ncbi.nlm.nih.gov/pubmed/11716089?tool=bestpractice.com
[36]St Jeor SC. Three-week incubation period for hantavirus infection. Pediatr Infect Dis J. 2004 Oct;23(10):974-5.
http://www.ncbi.nlm.nih.gov/pubmed/15602208?tool=bestpractice.com
However, symptoms of HCPS caused by ANDV typically appear within 4 to 42 days after exposure.[6]Centers for Disease Control and Prevention. 2026 multi-country hantavirus cluster linked to cruise ship. May 2026 [internet publication].
https://www.cdc.gov/han/php/notices/han00528.html
It should be noted that some patients with hantavirus infection may have milder illness without significant cardiopulmonary compromise.[57]UK Health Security Agency. Andes hantavirus: epidemiology, outbreaks and guidance. Jun 2026 [internet publication].
https://www.gov.uk/guidance/andes-hantavirus-epidemiology-outbreaks-and-guidance
Asymptomatic infection is thought to be rare in the US, but may be more common in Central and South America.[59]Ferrer JF, Jonsson CB, Esteban E, et al. High prevalence of hantavirus infection in Indian communities of the Paraguayan and Argentinean Gran Chaco. Am J Trop Med Hyg. 1998 Sep;59(3):438-44.
http://www.ajtmh.org/content/59/3/438.long
http://www.ncbi.nlm.nih.gov/pubmed/9749641?tool=bestpractice.com
[60]Campos GM, Moro de Sousa RL, Badra SJ, et al. Serological survey of hantavirus in Jardinopolis County, Brazil. J Med Virol. 2003 Nov;71(3):417-22.
http://www.ncbi.nlm.nih.gov/pubmed/12966548?tool=bestpractice.com
[61]Muñoz-Zanzi C, Saavedra F, Otth C, et al. Serological evidence of hantavirus infection in apparently healthy people from rural and slum communities in southern Chile. Viruses. 2015 Apr 17;7(4):2006-13.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4411687
http://www.ncbi.nlm.nih.gov/pubmed/25912713?tool=bestpractice.com
[62]Smith HM, Reporter R, Rood MP, et al. Prevalence study of antibody to ratborne pathogens and other agents among patients using a free clinic in downtown Los Angeles. J Infect Dis. 2002;186:1673-1676.
http://www.ncbi.nlm.nih.gov/pubmed/12447746?tool=bestpractice.com
[63]Yanagihara R. Hantavirus infection in the United States: epizootiology and epidemiology. Rev Infect Dis. 1990;12:449-457.
http://www.ncbi.nlm.nih.gov/pubmed/1972804?tool=bestpractice.com
Patients are typically only infectious when they are symptomatic.[6]Centers for Disease Control and Prevention. 2026 multi-country hantavirus cluster linked to cruise ship. May 2026 [internet publication].
https://www.cdc.gov/han/php/notices/han00528.html
Initial laboratory investigations
Specific investigations are usually not performed early in the illness. However, if a complete blood count (CBC) is performed for any reason (e.g., as part of the workup of a nonspecific viral illness), it may provide an early clue to the diagnosis, as thrombocytopenia with a supporting epidemiologic history is suggestive of hantavirus infection.[64]Chang B, Crowley M, Campen M, et al. Hantavirus cardiopulmonary syndrome. Semin Respir Crit Care Med. 2007 Apr;28(2):193-200.
http://www.ncbi.nlm.nih.gov/pubmed/17458773?tool=bestpractice.com
The presence of thrombocytopenia in the prodromal phase may indicate the need for confirmatory hantavirus testing.[65]Koster F, Foucar K, Hjelle B, et al. Rapid presumptive diagnosis of hantavirus cardiopulmonary syndrome by peripheral blood smear review. Am J Clin Pathol. 2001 Nov;116(5):665-72.
https://academic.oup.com/ajcp/article/116/5/665/1758184
http://www.ncbi.nlm.nih.gov/pubmed/11710682?tool=bestpractice.com
All patients with compatible symptoms should have a CBC performed.
CBC will show thrombocytopenia with an elevated hemoglobin (Hb) and hematocrit (Hct) as evidence of hemoconcentration. There is an associated leukocytosis with juvenile forms (immunoblasts).[5]Chapman LE, Ellis BA, Koster FT, et al. Discriminators between hantavirus-infected and -uninfected persons enrolled in a trial of intravenous ribavirin for presumptive hantavirus pulmonary syndrome. Clin Infect Dis. 2002 Feb 1;34(3):293-304.
http://cid.oxfordjournals.org/content/34/3/293.long
http://www.ncbi.nlm.nih.gov/pubmed/11774075?tool=bestpractice.com
The degree of thrombocytopenia may be prognostic of poor outcome.[10]Peters CJ, Khan AS. Hantavirus pulmonary syndrome: the new American hemorrhagic fever. Clin Infect Dis. 2002 May 1;34(9):1224-31.
https://academic.oup.com/cid/article/34/9/1224/463857
http://www.ncbi.nlm.nih.gov/pubmed/11941549?tool=bestpractice.com
The presence of 4 out of the 5 following findings after the onset of pulmonary edema has a sensitivity of 96% and specificity of 99% for HCPS:[65]Koster F, Foucar K, Hjelle B, et al. Rapid presumptive diagnosis of hantavirus cardiopulmonary syndrome by peripheral blood smear review. Am J Clin Pathol. 2001 Nov;116(5):665-72.
https://academic.oup.com/ajcp/article/116/5/665/1758184
http://www.ncbi.nlm.nih.gov/pubmed/11710682?tool=bestpractice.com
The combination of at least 4 of these findings can guide early management decisions until results of confirmatory tests are available.[65]Koster F, Foucar K, Hjelle B, et al. Rapid presumptive diagnosis of hantavirus cardiopulmonary syndrome by peripheral blood smear review. Am J Clin Pathol. 2001 Nov;116(5):665-72.
https://academic.oup.com/ajcp/article/116/5/665/1758184
http://www.ncbi.nlm.nih.gov/pubmed/11710682?tool=bestpractice.com
Confirmatory laboratory investigations
Testing to confirm the diagnosis is recommended in all patients with compatible symptoms and a relevant epidemiologic history.[66]Centres for Disease Control and Prevention. Clinician brief: hantavirus pulmonary syndrome (HPS). May 2026 [internet publication].
https://www.cdc.gov/hantavirus/hcp/clinical-overview/hps.html
Tests are typically available from local public health authorities, and consultation may be required for guidance on the type of testing to perform and the specimen types required. Specimens should be collected and handled according to local safety procedures.
Serologic testing is recommended to confirm the diagnosis.[57]UK Health Security Agency. Andes hantavirus: epidemiology, outbreaks and guidance. Jun 2026 [internet publication].
https://www.gov.uk/guidance/andes-hantavirus-epidemiology-outbreaks-and-guidance
[66]Centres for Disease Control and Prevention. Clinician brief: hantavirus pulmonary syndrome (HPS). May 2026 [internet publication].
https://www.cdc.gov/hantavirus/hcp/clinical-overview/hps.html
[67]World Health Organization. Hantavirus - fact sheet. May 2026 [internet publication].
https://www.who.int/news-room/fact-sheets/detail/hantavirus
[68]World Health Organization. Laboratory testing of Andes virus (Orthohantavirus andesense) infection: interim guidance, 15 May 2026. May 2026 [internet publication].
https://www.who.int/publications/i/item/B09765
Enzyme-linked immunosorbent assay (ELISA) immunoglobulin (Ig) M-capture and IgG serologies for hantavirus are recommended. ELISA or indirect immunofluorescence assay (IFA) may be used to confirm acute ANDV infection. However, the potential cross-reactivity with cocirculating hantaviruses should be considered, depending on local epidemiology.
Detection of hantavirus-specific IgM, or rising titers of hantavirus-specific IgG, confirms the diagnosis.[69]Centers for Disease Control and Prevention. Hantavirus pulmonary syndrome (HPS) 2015 case definition. Apr 2021 [internet publication].
https://ndc.services.cdc.gov/case-definitions/hantavirus-pulmonary-syndrome-2015
By the time the symptoms are evident, patients uniformly have antibodies of IgM class and some have antibodies of the IgG class.
Detection of hantavirus RNA by reverse transcriptase polymerase chain reaction (RT-PCR) may also be used.[57]UK Health Security Agency. Andes hantavirus: epidemiology, outbreaks and guidance. Jun 2026 [internet publication].
https://www.gov.uk/guidance/andes-hantavirus-epidemiology-outbreaks-and-guidance
[66]Centres for Disease Control and Prevention. Clinician brief: hantavirus pulmonary syndrome (HPS). May 2026 [internet publication].
https://www.cdc.gov/hantavirus/hcp/clinical-overview/hps.html
[67]World Health Organization. Hantavirus - fact sheet. May 2026 [internet publication].
https://www.who.int/news-room/fact-sheets/detail/hantavirus
[68]World Health Organization. Laboratory testing of Andes virus (Orthohantavirus andesense) infection: interim guidance, 15 May 2026. May 2026 [internet publication].
https://www.who.int/publications/i/item/B09765
[70]Vial C, Martinez-Valdebenito C, Rios S, et al. Molecular method for the detection of Andes hantavirus infection: validation for clinical diagnostics. Diagn Microbiol Infect Dis. 2016 Jan;84(1):36-9.
https://www.sciencedirect.com/science/article/pii/S0732889315002813
http://www.ncbi.nlm.nih.gov/pubmed/26508102?tool=bestpractice.com
RT-PCR is more sensitive in the early acute stages of illness (before antibodies appear), and is able to determine the specific species of hantavirus.
Identifying the species is important as enhanced IPC measures are required for ANDV infection due to the risk of human-to-human transmission.
RT-PCR testing on whole blood is recommended for confirmation of ANDV infection. If ANDV-specific assays are not available, sequencing is recommended to confirm the virus species.
A negative result does not rule out the diagnosis, particularly in the first 72 hours. Repeat testing should be considered 24 to 48 hours later (or up to 72 hours after, depending on guidance) if the clinical suspicion is high but initial testing is negative.[68]World Health Organization. Laboratory testing of Andes virus (Orthohantavirus andesense) infection: interim guidance, 15 May 2026. May 2026 [internet publication].
https://www.who.int/publications/i/item/B09765
[71]Centers for Disease Control and Prevention. About hantavirus. May 2024 [internet publication].
https://www.cdc.gov/hantavirus/about/index.html
Combining serology with RT-PCR is highly sensitive and represents a desirable approach to the laboratory diagnosis of HCPS, where available.[72]Machado AM, Figueiredo GG, Dos Santos Junior GS, et al. Laboratory diagnosis of human hantavirus infection: novel insights and future potential. Future Virol. 2009;4:383-9.
Investigations during cardiopulmonary phase
Once the cardiopulmonary phase begins, the disease can progress rapidly to cardiogenic shock and death and must be managed in an intensive care unit.[51]Jonsson CB, Hooper J, Mertz G. Treatment of hantavirus pulmonary syndrome. Antiviral Res. 2008 Apr;78(1):162-9.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2810485
http://www.ncbi.nlm.nih.gov/pubmed/18093668?tool=bestpractice.com
All patients should have a CBC, arterial blood gas (ABG), and serum lactate performed.
CBC shows hemoconcentration, as indicated by an elevated Hb and Hct.[65]Koster F, Foucar K, Hjelle B, et al. Rapid presumptive diagnosis of hantavirus cardiopulmonary syndrome by peripheral blood smear review. Am J Clin Pathol. 2001 Nov;116(5):665-72.
https://academic.oup.com/ajcp/article/116/5/665/1758184
http://www.ncbi.nlm.nih.gov/pubmed/11710682?tool=bestpractice.com
This is a marker for capillary leak.
ABG shows metabolic acidosis.[51]Jonsson CB, Hooper J, Mertz G. Treatment of hantavirus pulmonary syndrome. Antiviral Res. 2008 Apr;78(1):162-9.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2810485
http://www.ncbi.nlm.nih.gov/pubmed/18093668?tool=bestpractice.com
Elevated serum lactate levels are a marker of poor outcome.[73]Crowley MR, Katz RW, Kessler R, et al. Successful treatment of adults with severe Hantavirus pulmonary syndrome with extracorporeal membrane oxygenation. Crit Care Med. 1998 Feb;26(2):409-14. [Erratum in: Crit Care Med. 1998 Apr;26(4):806.]
http://www.ncbi.nlm.nih.gov/pubmed/9468181?tool=bestpractice.com
[74]Ulloa-Morrison R, Pavez N, Parra E, et al. Critical care management of hantavirus cardiopulmonary syndrome. A narrative review. J Crit Care. 2024 Dec;84:154867.
https://www.sciencedirect.com/science/article/pii/S088394412400354X?via%3Dihub
http://www.ncbi.nlm.nih.gov/pubmed/39024823?tool=bestpractice.com
Cardiac evaluation is also required.
Hemodynamic monitoring is important. The hemodynamic pattern of HCPS is not identical to septic or cardiogenic shock, and presents specific temporal patterns.[74]Ulloa-Morrison R, Pavez N, Parra E, et al. Critical care management of hantavirus cardiopulmonary syndrome. A narrative review. J Crit Care. 2024 Dec;84:154867.
https://www.sciencedirect.com/science/article/pii/S088394412400354X?via%3Dihub
http://www.ncbi.nlm.nih.gov/pubmed/39024823?tool=bestpractice.com
During the cardiopulmonary phase, a decreased cardiac index and increased peripheral resistance is seen, distinguishing the shock from septic shock, which has a low systemic resistance and high cardiac output. Peripheral resistance and cardiac index is assessed using a flow-directed pulmonary artery catheter (Swan-Ganz catheter). Alternative methods (e.g., transpulmonary thermodilution catheter) may be available in specialist centers. A cardiac index of <2.5 L/minute/m² is one of the criteria for instituting extracorporeal membrane oxygenation (ECMO).[58]Mertz GJ, Hjelle B, Crowley M, et al. Diagnosis and treatment of new world hantavirus infections. Curr Opin Infect Dis. 2006 Oct;19(5):437-42.
http://www.ncbi.nlm.nih.gov/pubmed/16940866?tool=bestpractice.com
[73]Crowley MR, Katz RW, Kessler R, et al. Successful treatment of adults with severe Hantavirus pulmonary syndrome with extracorporeal membrane oxygenation. Crit Care Med. 1998 Feb;26(2):409-14. [Erratum in: Crit Care Med. 1998 Apr;26(4):806.]
http://www.ncbi.nlm.nih.gov/pubmed/9468181?tool=bestpractice.com
[74]Ulloa-Morrison R, Pavez N, Parra E, et al. Critical care management of hantavirus cardiopulmonary syndrome. A narrative review. J Crit Care. 2024 Dec;84:154867.
https://www.sciencedirect.com/science/article/pii/S088394412400354X?via%3Dihub
http://www.ncbi.nlm.nih.gov/pubmed/39024823?tool=bestpractice.com
[75]Hallin GW, Simpson SQ, Crowell RE, et al. Cardiopulmonary manifestations of hantavirus pulmonary syndrome. Crit Care Med. 1996 Feb;24(2):252-8.
http://www.ncbi.nlm.nih.gov/pubmed/8605797?tool=bestpractice.com
Lung biopsy may be performed either transbronchially at bronchoscopy or by video-assisted thoracoscopic surgery in patients with unexplained rapidly progressive pulmonary disease.[75]Hallin GW, Simpson SQ, Crowell RE, et al. Cardiopulmonary manifestations of hantavirus pulmonary syndrome. Crit Care Med. 1996 Feb;24(2):252-8.
http://www.ncbi.nlm.nih.gov/pubmed/8605797?tool=bestpractice.com
[76]Nolte KB, Feddersen RM, Foucar K, et al. Hantavirus pulmonary syndrome in the United States: a pathological description of a disease caused by a new agent. Hum Pathol. 1995 Jan;26(1):110-20.
http://www.ncbi.nlm.nih.gov/pubmed/7821907?tool=bestpractice.com
In cases of HCPS it will show intra-alveolar edema with an interstitial infiltrate of immunoblasts. There will be scant polymorphonuclear cells. Endothelial and alveolar lining cells are intact and appear normal.
Immunohistochemical staining for hantavirus RNA is available as a research test through the CDC and will show diffuse endothelial cell staining.
Imaging
All patients with respiratory symptoms should have a chest x-ray (CXR) performed.[5]Chapman LE, Ellis BA, Koster FT, et al. Discriminators between hantavirus-infected and -uninfected persons enrolled in a trial of intravenous ribavirin for presumptive hantavirus pulmonary syndrome. Clin Infect Dis. 2002 Feb 1;34(3):293-304.
http://cid.oxfordjournals.org/content/34/3/293.long
http://www.ncbi.nlm.nih.gov/pubmed/11774075?tool=bestpractice.com
[77]Boroja M, Barrie JR, Raymond GS. Radiographic findings in 20 patients with Hantavirus pulmonary syndrome correlated with clinical outcome. AJR Am J Roentgenol. 2002 Jan;178(1):159-63.
http://www.ajronline.org/cgi/content/full/178/1/159
http://www.ncbi.nlm.nih.gov/pubmed/11756112?tool=bestpractice.com
In the early pulmonary phase, CXR may be normal or suggestive of early interstitial edema.
In the cardiopulmonary phase, CXR shows evidence of progressive noncardiogenic pulmonary edema (the heart size remains normal and pulmonary infiltrates with or without pleural effusion may be present).[Figure caption and citation for the preceding image starts]: Bilateral fluffy pulmonary infiltrates in hantavirus pulmonary syndromeCDC Public Health Image Library (PHIL), Loren Ketai, MD [Citation ends].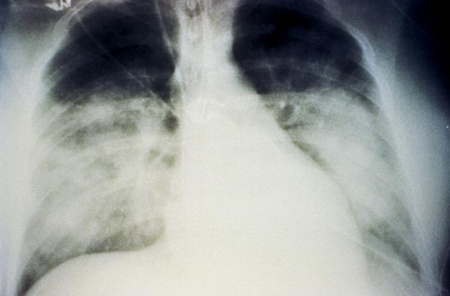
Emerging investigations
Hantavirus isolation in cell culture is not routinely recommended for laboratory diagnosis. Virus isolation requires specialized expertise and Biosafety 3 laboratory facilities. Nevertheless, ANDV has been isolated in cell culture from the blood of patients and from organs of those with fatal disease.[4]Figueiredo LT, Souza WM, Ferrés M, et al. Hantaviruses and cardiopulmonary syndrome in South America. Virus Res. 2014 Jul 17;187:43-54.
http://www.ncbi.nlm.nih.gov/pubmed/24508343?tool=bestpractice.com
There are currently no antigen-based rapid diagnostic tests available.
Differential diagnosis
Symptoms of early infection are nonspecific and can resemble many other febrile and respiratory illnesses, and the differential diagnosis is broad. Testing for more common illnesses (e.g., influenza, coronavirus disease 2019 [COVID-19], and other common causes of febrile and gastrointestinal illnesses) is recommended in an acutely unwell patient with epidemiologic risk factors and compatible symptoms.[6]Centers for Disease Control and Prevention. 2026 multi-country hantavirus cluster linked to cruise ship. May 2026 [internet publication].
https://www.cdc.gov/han/php/notices/han00528.html
