小结
鉴别诊断
常见
- 消化性溃疡 (PUD)
- 食管静脉曲张
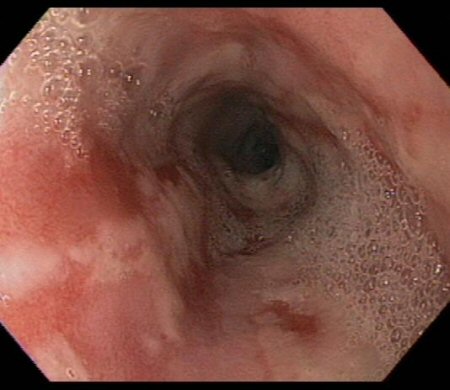
- 食管炎
- Mallory-Weiss 撕裂
不常见
- Boerhaave 综合征(自发性食管穿孔)
- 胃底静脉曲张
- 动静脉畸形 (Arteriovenous malformations, AVMs)
- Dieulafoy 病
- 上消化道肿瘤
- 主动脉消化道瘘 (Aortoenteric fistulae, AEF)
- 凝血功能障碍
撰稿人
作者
Douglas G. Adler, MD, FACG, AGAF, FASGE
Professor of Medicine
Director, Gastrointestinal Fellowship Program
Director of Therapeutic Endoscopy
Division of Gastroenterology
Department of Internal Medicine
Huntsman Cancer Institute
University of Utah
Salt Lake City
UT
利益声明
DGA has consulted for Boston Scientific and Merit Medical, which make endoscopic retrograde cholangiopancreatography (ERCP) products. He is also an author of references cited in this topic.
鸣谢
Dr Douglas G. Adler would like to gratefully acknowledge the assistance of Dr Patrick D. Martin.
利益声明
PDM declares that he has no competing interests.
同行评议者
Ned Snyder, MD, FACP
Professor of Medicine
Chief of Clinical Gastroenterology and Hepatology
University of Texas Medical Branch
Galveston
TX
利益声明
NS declares that he has no competing interests.
David J. Hackam, MD, PhD
Associate Professor of Pediatric Surgery
University of Pittsburgh School of Medicine
Pittsburgh
PA
利益声明
DJH declares that he has no competing interests.
Giuseppe Malizia, MD
Consultant Gastroenterologist
Divisione di Gastroenterologia
Ospedale V. Cervello
Palermo
Italy
利益声明
GM declares that he has no competing interests.
指南
- 大出血的血液学管理
- 上消化道出血和溃疡出血
更多 指南患者教育信息
烧心
GORD:询问医生
更多 患者教育信息医学计算器
上消化道出血的 Rockall 评分
胃肠道出血的 Blatchford 评分
更多 医学计算器Videos
静脉穿刺和抽血的动画演示
更多 操作视频 登录或订阅即可浏览 BMJ Best Practice 临床实践完整内容
登录或订阅即可浏览 BMJ Best Practice 临床实践完整内容
内容使用需遵循免责声明