Resumo
Definição
História e exame físico
Principais fatores diagnósticos
- náuseas e vômitos
- distensão abdominal
- ausência de características de obstrução mecânica ou de inflamação peritoneal (por exemplo, hérnia abdominal, sinais peritoneais)
Outros fatores diagnósticos
- obstipação (constipação grave, sem passagem de fezes ou flatos)
- desconforto e cólica abdominal
- ruídos hidroaéreos reduzidos ou hipoativos
- hipovolemia
Fatores de risco
- cirurgia abdominal
- doença aguda/sistêmica (por exemplo, infarto do miocárdio [IAM], pneumonia, colecistite aguda, pancreatite, sepse, trauma de múltiplos órgãos)
- cirurgia não abdominal
- desequilíbrio eletrolítico
- analgésicos opioides, anticolinérgicos ou gases anestésicos
- comorbidades (por exemplo, diabetes mellitus, insuficiência cardiovascular, doença de Chagas, esclerodermia)
Investigações diagnósticas
Primeiras investigações a serem solicitadas
- eletrólitos séricos
- magnésio sérico
- Hemograma completo
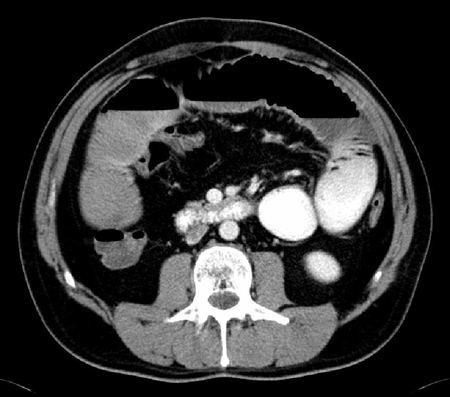
- tomografia computadorizada (TC) do abdome e da pelve (com contraste intravenoso e contraste oral hidrossolúvel)
Investigações a serem consideradas
- testes séricos da função hepática
- amilase sérica
- lipase sérica
- radiografias do intestino delgado
- estudo de esvaziamento gástrico
Algoritmo de tratamento
íleo paralítico pós-operatório
causa não cirúrgica
íleo paralítico que dure mais de 3 dias ou que prolongue a recuperação pós-operatória
Colaboradores
Autores
Steven D. Wexner, MD, PhD (Hon), FACS, FRCS (Eng), FRCS (Ed), FRCSI (Hon)

Director
Digestive Disease Center
Professor and Chair
Department of Colorectal Surgery
Cleveland Clinic
Weston
FL
Declarações
SDW has received consulting fees, stock options, and royalties from the following companies. These relationships are ongoing. Consulting: ICON Language Services, Intuitive Surgical, Stryker, Medtronic, Takeda, ARC/Corvus, Astellas, Baxter, Olympus, AIS Channel, Livsmed. Royalties: Medtronic, Intuitive Surgical, Karl Storz Endoscopy-America, Unique Surgical Innovations. Stock Options: Regentys, LifeBond, Pragma/GibLib, and Renew Medical.
Sameh Hany Emile Rizkalla, MBBCh, MSc, MD, FACS
Research associate, Colorectal Surgery Department
Digestive Disease Center
Professor and Chair
Department of Colorectal Surgery
Cleveland Clinic
Weston
FL
Declarações
SHER declares that he has no competing interests.
Agradecimentos
Dr Steven D. Wexner would like to gratefully acknowledge the contribution of Dr Stephen P. Sharp to the update for this topic. Dr Wexner would also like to acknowledge Dr Ahmed Sami Chadi, and Dr Paula I. Denoya, previous contributors to this topic.
Declarações
SPS, ASC, and PID declare that they have no competing interests.
Revisores
David J. Hackam, MD, PhD
Associate Professor of Pediatric Surgery
University of Pittsburgh School of Medicine
Pittsburgh
PA
Declarações
DJH declares that he has no competing interests.
John Jenkins, MB CHB, FRCP
Consultant Colorectal Surgeon
St. Mark's Hospital
Harrow
UK
Declarações
JJ declares that he has no competing interests.
Créditos aos pareceristas
Os tópicos do BMJ Best Practice são constantemente atualizados, seguindo os desenvolvimentos das evidências e das diretrizes. Os pareceristas aqui listados revisaram o conteúdo pelo menos uma vez durante a história do tópico.
Declarações
As afiliações e declarações dos pareceristas referem--se ao momento da revisão.
Referências
Principais artigos
Wattchow D, Heitmann P, Smolilo D, et al. Postoperative ileus-an ongoing conundrum. Neurogastroenterol Motil. 2021 May;33(5):e14046. Resumo
Gustafsson UO, Scott MJ, Hubner M, et al. Guidelines for perioperative care in elective colorectal surgery: Enhanced Recovery After Surgery (ERAS(®)) Society recommendations: 2018. World J Surg. 2019 Mar;43(3):659-95.Texto completo Resumo
American College of Radiology. ACR Appropriateness Criteria: suspected small-bowel obstruction. 2019 [internet publication].Texto completo
Artigos de referência
Uma lista completa das fontes referenciadas neste tópico está disponível para os usuários com acesso total ao BMJ Best Practice.
Diagnósticos diferenciais
- Obstrução intestinal mecânica
- Pseudo-obstrução (síndrome de Ogilvie)
- Gastroenterite
Mais Diagnósticos diferenciaisDiretrizes
- ACR appropriateness criteria: suspected small-bowel obstruction
- American Society for Enhanced Recovery and Perioperative Quality Initiative joint consensus statement on postoperative gastrointestinal dysfunction within an enhanced recovery pathway for elective colorectal surgery
Mais DiretrizesVideos
Demonstração animada da inserção de sonda nasogástrica
Mais vídeos Conectar-se ou assinar para acessar todo o BMJ Best Practice
Conectar-se ou assinar para acessar todo o BMJ Best Practice
O uso deste conteúdo está sujeito ao nosso aviso legal