Resumo
Definição
Os meniscos medial e lateral, localizados entre o fêmur e a tíbia, absorvem o choque e distribuem a força. Consequentemente, os meniscos podem se romper devido a lesão traumática ou desgaste degenerativo (por exemplo na artrose do joelho), e podem comprometer a distribuição da força em toda a articulação do joelho. Uma ruptura do menisco ocorre em 2 planos primários: vertical e horizontal. As rupturas verticais geralmente resultam de um trauma agudo, enquanto as rupturas horizontais geralmente são de natureza degenerativa.[1]As rupturas podem causar dor, edema, limitação da amplitude de movimentos e travamento, bloqueio e instabilidade da articulação do joelho. As rupturas podem causar alterações artríticas degenerativas, se já não estiverem presentes.
[Figure caption and citation for the preceding image starts]: Estruturas anatômicas em volta dos meniscosCriado por BMJ Publishing Group [Citation ends].
História e exame físico
Principais fatores diagnósticos
- presença de fatores de risco
- edema no joelho
- sensação de instabilidade ou perda de apoio repentina/travamento do joelho
- dor no joelho
- sensibilidade e crepitação na interlinha articular
Outros fatores diagnósticos
- cisto poplíteo (cisto de Baker) em casos crônicos
- amplitude de movimentos limitada
Fatores de risco
- trauma agudo (lesão por torção)
- artrite do joelho
- instabilidade do joelho
- história de lesão do ligamento cruzado anterior
- desalinhamento da articulação do joelho
- superfície irregular ou desigual para prática esportiva
- condições de solo/meteorológicas desfavoráveis
- idade avançada
- trabalhos manuais e na construção civil
- menisco discoide
- índice de massa corporal (IMC) alto
Investigações diagnósticas
Primeiras investigações a serem solicitadas
- testes clínicos
- ressonância nuclear magnética (RNM)
- radiografia
Investigações a serem consideradas
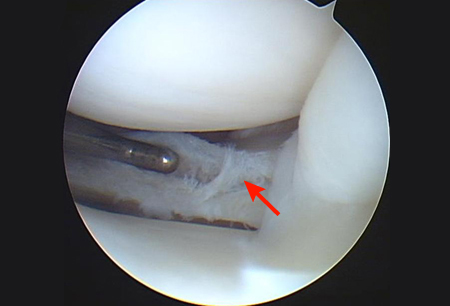
- artroscopia
- artrografia por tomografia computadorizada (TC)
- ultrassonografia
Algoritmo de tratamento
todos os pacientes
Colaboradores
Autores
Hideki Takeda, MD
Orthopedic Surgeon
Department of Sports Orthopedics
NTT Medical Center Tokyo
Tokyo
Japan
Declarações
HT declares that he has no competing interests.
Agradecimentos
Dr Hideki Takeda would like to gratefully acknowledge Dr Lars Engebretsen and Dr Kevin R. Stone, previous contributors to this topic.
Declarações
LE declares that he has no competing interests. KRS is an author of several references cited in this topic.
Revisores
Daniel Solomon, MD
Co-Director of Orthopedic Sports and Shoulder Service
Department of Orthopedic Surgery
Naval Medical Center San Diego
San Diego
CA
Declarações
DS declares that he has no competing interests.
Jung-Ro Yoon, MD
Orthopedic Surgeon
Department of Orthopedic Surgery
Seoul Veterans Hospital
Seoul
South Korea
Declarações
JRY declares that she has no competing interests.
Nikunj N. Trivedi, MD
Fellow
Sports Medicine and Shoulder Surgery
Stanford University
Stanford
CA
Declarações
NNT declares that he has no competing interests.
Seth L. Sherman, MD
Associate Professor of Orthopedic Surgery
Fellowship Director
Sports Medicine and Shoulder Surgery
Stanford University
Stanford
CA
Declarações
SLS declares that he has no competing interests.
Créditos aos pareceristas
Os tópicos do BMJ Best Practice são constantemente atualizados, seguindo os desenvolvimentos das evidências e das diretrizes. Os pareceristas aqui listados revisaram o conteúdo pelo menos uma vez durante a história do tópico.
Declarações
As afiliações e declarações dos pareceristas referem--se ao momento da revisão.
Referências
Principais artigos
Kopf S, Beaufils P, Hirschmann MT, et al. Management of traumatic meniscus tears: the 2019 ESSKA meniscus consensus. Knee Surg Sports Traumatol Arthrosc. 2020 Apr;28(4):1177-94.Texto completo Resumo
American Physical Therapy Association. Knee pain and mobility impairments: meniscal and articular cartilage lesions, revision 2018. 2018 [internet publication].
American College of Radiology. ACR Appropriateness Criteria® acute trauma to the knee. 2019 [internet publication].Texto completo
Artigos de referência
Uma lista completa das fontes referenciadas neste tópico está disponível para os usuários com acesso total ao BMJ Best Practice.
Diagnósticos diferenciais
- Ruptura do ligamento cruzado anterior
- Entorse do ligamento colateral medial
- Entorse do ligamento cruzado posterior
Mais Diagnósticos diferenciaisDiretrizes
- Acute isolated meniscal pathology
- Management of traumatic meniscus tears: the 2019 ESSKA meniscus consensus
Mais Diretrizes Conectar-se ou assinar para acessar todo o BMJ Best Practice
Conectar-se ou assinar para acessar todo o BMJ Best Practice
O uso deste conteúdo está sujeito ao nosso aviso legal