Resumo
Definição
Placenta prévia (PP) é definida como a placenta que se sobrepõe ao óstio cervical.[1][2][3] A PP diagnosticada no segundo trimestre provavelmente se resolverá com o decorrer da gestação.[1][3] Em mulheres com um útero cicatrizado (mais comumente proveniente de um parto cesáreo anterior), a PP pode estar associada ao espectro da placenta acreta (anteriormente conhecido como placenta anormalmente aderente e placenta morbidamente aderente), em que a placenta se liga à camada miometrial do útero.[4] Vasa prévia, onde os vasos fetais se sobrepõem ao óstio cervical interno, é uma condição associada.[5]
Neste tópico, referimo-nos a todas as variedades de placentação invasiva como no espectro da placenta acreta.[4] Existem três variações comumente definidas: placenta acreta (em que as vilosidades coriônicas se ligam ao miométrio, em vez de estarem restritas ao interior da decídua basal), placenta increta (em que as vilosidades coriônicas invadem o miométrio) e placenta percreta (em que as vilosidades coriônicas invadem o miométrio e, às vezes, o tecido contíguo).[4] Embora essas distinções sejam importantes para os especialistas, elas não alteram as decisões de manejo para os profissionais de atenção primária.[Figure caption and citation for the preceding image starts]: Placenta prévia (anteriormente conhecida como prévia total) na 22ª semanaDo acervo de aulas de Janet R. Albers, MD [Citation ends].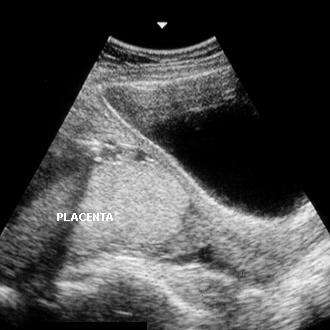
História e exame físico
Principais fatores diagnósticos
- útero cicatrizado
- presença de outros fatores de risco
- sangramento vaginal indolor
- ausência de causas cervicais/vaginais de sangramento no exame especular
Outros fatores diagnósticos
- anomalia na ultrassonografia prévia no primeiro trimestre
- falta de sensibilidade uterina
- hipotensão arterial e taquicardia
Fatores de risco
- idade materna avançada
- múltiplas gestações prévias
- tabagismo
- aborto espontâneo prévio
- aborto induzido prévio
- outras anormalidades placentárias
- intervalos curtos entre gestações
- uso de substâncias ilícitas
- cicatrização uterina (mais comumente decorrente de um parto cesáreo prévio)
- tratamentos para infertilidade
- placenta prévia anterior
Investigações diagnósticas
Primeiras investigações a serem solicitadas
- ultrassonografia uterina com análise com dopplerfluxometria colorida
- Hemograma completo
- tipagem sanguínea e prova cruzada
Investigações a serem consideradas
- ressonância nuclear magnética (RNM) da placenta
- razão normalizada internacional/tempo de tromboplastina parcial (INR/TTP), fibrinogênio e produtos de degradação do fibrinogênio
- teste de Kleihauer-Betke
Algoritmo de tratamento
sangramento com posição da placenta desconhecida
sangramento com posição da placenta prévia conhecida
placenta prévia sem sangramento
com aborto espontâneo ou interrupção eletiva
Colaboradores
Autores
Janet R. Albers, MD

Professor
Department Chair
Family and Community Medicine
Southern Illinois University School of Medicine
Springfield
IL
Declarações
JRA declares that she has no competing interests.
Thomas H. Miller, MD
Professor
Clinical Family and Community Medicine
Associate Chairman - Western Region
Southern Illinois University School of Medicine
Springfield
IL
Declarações
THM declares that he has no competing interests.
Agradecimentos
Dr Janet R. Albers and Dr Thomas H. Miller would like to gratefully acknowledge Dr Robert Ewart and Dr Matthew Hagermeyer, previous contributors to this topic.
Declarações
RE and MH declare that they have no competing interests.
Revisores
Yosra Tahir Jarjees, MD
Assistant Professor
Head of Department of Obstetrics and Gynecology
Mosul College of Medicine
Mosul
Iraq
Declarações
YTJ declares that he has no competing interests.
John Bachman, MD
Consultant in Family Medicine
Parker D Sanders and Isabella Sanders Professor of Primary Care
Rochester
MN
Declarações
JB declares that he has no competing interests.
Créditos aos pareceristas
Os tópicos do BMJ Best Practice são constantemente atualizados, seguindo os desenvolvimentos das evidências e das diretrizes. Os pareceristas aqui listados revisaram o conteúdo pelo menos uma vez durante a história do tópico.
Declarações
As afiliações e declarações dos pareceristas referem--se ao momento da revisão.
Referências
Principais artigos
Jain V, Bos H, Bujold E; Society of Obstetricians and Gynaecologists of Canada. Guideline no. 402: diagnosis and management of placenta previa. J Obstet Gynaecol Can. 2020 Jul;42(7):906-17.e1. Resumo
Royal College of Obstetricians and Gynaecologists. Placenta praevia and placenta accreta: diagnosis and management. Green-top guideline no. 27a. Sep 2018 [internet publication].Texto completo
American College of Obstetricians and Gynecologists / Society for Maternal-Fetal Medicine. ACOG SMFM obstetric care consensus #7: placenta accreta spectrum. Dec 2018 [internet publication].Texto completo
Shipp TD, Poder L, Feldstein VA, et al; Expert Panel on GYN and OB Imaging, American College of Radiology. ACR appropriateness criteria: second and third trimester vaginal bleeding. J Am Coll Radiol. 2020 Nov;17(11s):S497-504.Texto completo Resumo
Artigos de referência
Uma lista completa das fontes referenciadas neste tópico está disponível para os usuários com acesso total ao BMJ Best Practice.
Diagnósticos diferenciais
- Trabalho de parto normal
- Descolamento da placenta
- Aborto espontâneo
Mais Diagnósticos diferenciaisDiretrizes
- Caesarean birth
- Guideline no. 402: diagnosis and management of placenta previa
Mais Diretrizes Conectar-se ou assinar para acessar todo o BMJ Best Practice
Conectar-se ou assinar para acessar todo o BMJ Best Practice
O uso deste conteúdo está sujeito ao nosso aviso legal