Resumo
Definição
História e exame físico
Principais fatores diagnósticos
- presença de fatores de risco
- a dor é exacerbada pela atividade
- local da dor na região anteromedial do joelho com o joelho fletido a 90°
- local da dor na região lateral do cotovelo
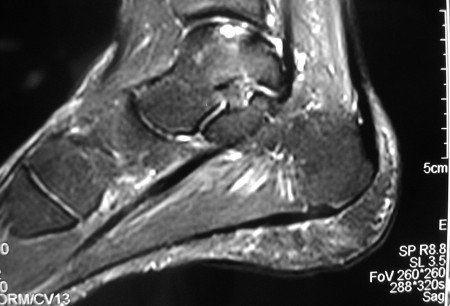
- local da dor na região posteromedial do tornozelo dorsifletido ou região anterolateral do tornozelo em flexão plantar
- presença de derrame
- bloqueio da articulação
- travamento da articulação
- amplitude de movimentos reduzida
Outros fatores diagnósticos
- comprometimento do joelho, idade de 10 a 20 anos
- comprometimento do cotovelo, idade entre 11 a 21 anos
- comprometimento do tálus, da segunda à quarta década
- ausência de história de trauma envolvendo o joelho ou cotovelo
- marcha antálgica na osteocondrite dissecante comprometendo o joelho ou tálus
- marcha de rotação externa na osteocondrite dissecante comprometendo o joelho
- fatores de alívio: anti-inflamatórios não esteroidais (AINEs), repouso, gelo, elevação
- crepitação
- teste de Wilson
- atrofia do quadríceps
Fatores de risco
- estresse valgo/arremesso repetitivo
- ginástica/levantamento de peso nos membros superiores
- entorse/instabilidade do tornozelo
- atividades atléticas competitivas
- história familiar
Investigações diagnósticas
Primeiras investigações a serem solicitadas
- radiografias do joelho
- radiografias do tornozelo
- radiografia panorâmica do membro inferior
- radiografias do cotovelo
Investigações a serem consideradas
- tomografia computadorizada (TC)
- RNM
- Artrorressonância
- artroscopia diagnóstica
Algoritmo de tratamento
joelho
cotovelo
tornozelo (tálus)
Colaboradores
Autores
Henry G. Chambers, MD
Professor of Clinical Orthopedic Surgery
University of California, San Diego
Rady Children’s Hospital
San Diego
CA
Declarações
HGC is an author of a number of references cited in this topic.
Agradecimentos
Dr Henry G. Chambers would like to gratefully acknowledge Dr James L. Carey, Dr Jon Divine, Dr Michael Nett, and Dr Cedric Ortiguera, the previous contributors to this topic.
Declarações
JLC is an author of a number of references cited in this topic. JD, MN, and CO declared that they had no competing interests.
Revisores
James E. McGrory, MD
Orthopedic Surgeon
The Hughston Clinic PC
Columbus
GA
Declarações
JEM declares that he has no competing interests.
Nicola Maffulli, MD, MS, PhD, FRCS(Orth)
Centre Lead and Professor of Sports and Exercise Medicine
Consultant Trauma and Orthopaedic Surgeon
Barts and The London School of Medicine and Dentistry
Institute for Health Sciences Education
Centre for Sports and Exercise Medicine
Queen Mary University of London
Mile End Hospital
London
UK
Declarações
NM declares that he has no competing interests.
Créditos aos pareceristas
Os tópicos do BMJ Best Practice são constantemente atualizados, seguindo os desenvolvimentos das evidências e das diretrizes. Os pareceristas aqui listados revisaram o conteúdo pelo menos uma vez durante a história do tópico.
Declarações
As afiliações e declarações dos pareceristas referem--se ao momento da revisão.
Referências
Principais artigos
Kocher MS, Tucker R, Ganley TJ, et al. Management of osteochondritis dissecans of the knee: current concepts review. Am J Sports Med. 2006 Jul;34(7):1181-91. Resumo
American Academy of Orthopaedic Surgeons. Diagnosis and treatment of osteochondritis dissecans. Dec 2023 [internet publication].Texto completo
Perumal V, Wall E, Babekir N. Juvenile osteochondritis dissecans of the talus. J Pediatr Orthop. 2007 Oct-Nov;27(7):821-5. Resumo
Baker CL 3rd, Baker CL Jr, Romeo AA. Osteochondritis dissecans of the capitellum. Am J Sports Med. 2010 Sep;38(9):1917-28. Resumo
Artigos de referência
Uma lista completa das fontes referenciadas neste tópico está disponível para os usuários com acesso total ao BMJ Best Practice.
Diagnósticos diferenciais
- Fratura osteocondral
- Ruptura do menisco
- Artrite séptica
Mais Diagnósticos diferenciaisDiretrizes
- Osteochondritis dissecans: diagnosis and treatment
Mais Diretrizes Conectar-se ou assinar para acessar todo o BMJ Best Practice
Conectar-se ou assinar para acessar todo o BMJ Best Practice
O uso deste conteúdo está sujeito ao nosso aviso legal