Resumo
Definição
História e exame físico
Principais fatores diagnósticos
- presença de fatores de risco
- diarreia
- perda de peso
- artralgia
- oftalmoplegia supranuclear
Outros fatores diagnósticos
- dor abdominal
- linfadenopatia
- febre
- esteatorreia
- anemia
- escurecimento da pele
- confusão, comprometimento da memória, alteração do nível de consciência ou demência
- apatia
- ansiedade, depressão, hipomania, psicose, alteração de personalidade
- sinais mioclônicos
- convulsões
- nistagmo
- reflexos vivos, reflexos cutâneo-plantares em extensão, fraqueza predominante em músculos extensores dos braços e flexores das pernas, hipertonia
- amenorreia, polidipsia, hiperfagia, diminuição da libido
- ataxia
- cefaleias
- miorritmias oculomastigatória e oculofacioesquelética
- hemiparesia
- comprometimento de nervos cranianos
- distúrbio do movimento extrapiramidal
- neuropatias periféricas
Fatores de risco
- idade >50 anos
- sexo masculino
- fatores genéticos
Investigações diagnósticas
Primeiras investigações a serem solicitadas
- Hemograma completo
- albumina sérica
- proteína C-reativa sérica
- velocidade de hemossedimentação (VHS) sérica
- endoscopia digestiva alta
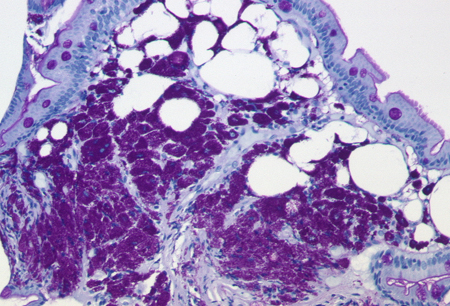
- coloração de biópsias duodenais com ácido periódico de Schiff (PAS)
- reação em cadeia da polimerase
- Imuno-histoquímica específica para Tropheryma whipplei
Novos exames
- microscopia eletrônica
- cultura
- sorologia
Algoritmo de tratamento
pacientes sem comprometimento do sistema nervoso central (SNC)
pacientes com comprometimento do sistema nervoso central (SNC)
Colaboradores
Autores
Thomas Schneider, MD, PhD
Professor
Medical Department I
Charité - University Medicine Berlin
CBF
Berlin
Germany
Declarações
TS is an author of a number of references cited in this topic.
Verena Moos, PhD
Scientist
Medical Department I
Charité - University Medicine Berlin
CBF
Berlin
Germany
Declarações
VM is an author of a number of references cited in this topic.
Revisores
Stephen G. Baum, MD
Professor of Medicine
Department of Microbiology and Immunology
Albert Einstein College of Medicine
Bronx
NY
Declarações
SGB declares that he has no competing interests.
Chris Huston, MD
Assistant Professor of Medicine
Division of Infectious Diseases
University of Vermont
Burlington
VT
Declarações
CH declares that he has no competing interests.
Créditos aos pareceristas
Os tópicos do BMJ Best Practice são constantemente atualizados, seguindo os desenvolvimentos das evidências e das diretrizes. Os pareceristas aqui listados revisaram o conteúdo pelo menos uma vez durante a história do tópico.
Declarações
As afiliações e declarações dos pareceristas referem--se ao momento da revisão.
Referências
Principais artigos
Schneider T, Moos V, Loddenkemper C, et al. Whipple's disease: new aspects of pathogenesis and treatment. Lancet Infect Dis. 2008 Mar;8(3):179-90. Resumo
Fenollar F, Puechal X, Raoult D. Whipple's disease. N Engl J Med. 2007 Jan 4;356(1):55-66.
Dobbins WO. Whipple's disease. Springfield, IL: Thomas; 1987.
Louis ED, Lynch T, Kaufmann P, et al. Diagnostic guidelines in central nervous system Whipple's disease. Ann Neurol. 1996 Oct;40(4):561-8. Resumo
Feurle GE, Junga NS, Marth T. Efficacy of ceftriaxone or meropenem as initial therapies in Whipple's disease. Gastroenterology. 2010 Feb;138(2):478-86; quiz 11-2.Texto completo Resumo
Feurle GE, Moos V, Bläker H, et al. Intravenous ceftriaxone, followed by 12 or three months of oral treatment with trimethoprim-sulfamethoxazole in Whipple's disease. J Infect. 2013 Mar;66(3):263-70. Resumo
Artigos de referência
Uma lista completa das fontes referenciadas neste tópico está disponível para os usuários com acesso total ao BMJ Best Practice.
Diagnósticos diferenciais
- Artrite reumatoide soronegativa
- Sarcoidose
- Doença celíaca
Mais Diagnósticos diferenciaisFolhetos informativos para os pacientes
Diarreia em adultos
Diarreia em crianças
Mais Folhetos informativos para os pacientes Conectar-se ou assinar para acessar todo o BMJ Best Practice
Conectar-se ou assinar para acessar todo o BMJ Best Practice
O uso deste conteúdo está sujeito ao nosso aviso legal