Summary
Definition
History and exam
Key diagnostic factors
- idade entre 20 e 50 anos
- sexo feminino
- dispneia
- componente pulmonar (P2) acentuado na segunda bulha cardíaca
- sopro de regurgitação tricúspide
- história familiar
Other diagnostic factors
- fadiga
- edema periférico
- cianose
- uso de estimulantes
- síncope
- dor torácica
- pré-síncope
- sopro diastólico precoce agudo na área pulmonar
- distensão jugular
Risk factors
- história familiar
- sexo feminino
- mutações do receptor da proteína morfogenética óssea tipo 2 (BMPR2)
- redutores de apetite
- drogas e toxinas
Diagnostic tests
1st tests to order
- radiografia torácica
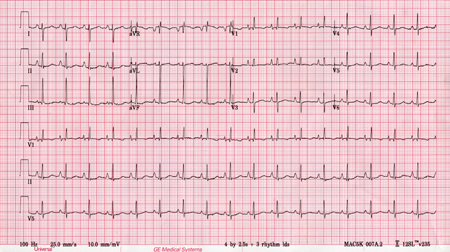
- eletrocardiograma (ECG)
- ecocardiografia transtorácica com Doppler
- cateterismo cardíaco direito
- fatores antinucleares (FANs)
- testes de função pulmonar
- gasometria arterial
- oximetria noturna
- cintilografia de ventilação/perfusão (V/Q)
- teste de caminhada de 6 minutos
- Peptídeo natriurético do tipo B (PNB) ou pró-peptídeo natriurético do tipo B N-terminal (NT-proPNB)
- Hemograma completo
- TFHs
- testes da função tireoidiana
- sorologia do HIV
Tests to consider
- tomografia computadorizada (TC) de alta resolução do tórax ± angiografia pulmonar por TC
- ressonância nuclear magnética (RNM) cardíaca
- teste de vasodilatação com óxido nítrico por via inalatória, iloprosta por via inalatória ou epoprostenol intravenoso
Treatment algorithm
resposta positiva ao teste de vasorreatividade aguda sem contraindicação a bloqueadores dos canais de cálcio
resposta negativa ao teste de vasorreatividade aguda ou contraindicação a bloqueadores dos canais de cálcio: sem comorbidade cardiopulmonarm
Contributors
Authors
Muhammad Sameed, MD
Director Advance Lung Disease Program
Department of Pulmonary & Critical Care Medicine
Assistant professor of Medicine
Thomas Jefferson University Hospital - Einstein Health
Philadelphia
PA
Disclosures
MS declares that he has no competing interests.
Gustavo A. Heresi, MD, MS

Director, Pulmonary Vascular and CTEPH Program
Department of Pulmonary and Critical Care Medicine
Respiratory Institute
Cleveland Clinic
Cleveland
OH
Disclosures
GAH has received speaking and advisory board fees from Bayer Healthcare, the manufacturer of riociguat.
Acknowledgements
Dr Muhammad Sameed and Dr Gustavo A. Heresi would like to gratefully acknowledge Dr Raed A. Dweik, a previous contributor to this topic.
Disclosures
RAD declares that he has no competing interests.
Peer reviewers
Michael J. Krowka, MD
Division of Pulmonary and Critical Care Medicine
Mayo Clinic College of Medicine
Rochester
MN
Disclosures
MJK declares that he has no competing interests.
Charlie Elliot, MB ChB, MRCP
Consultant Physician in Respiratory and General Internal Medicine
Sheffield Pulmonary Vascular Disease Unit
Royal Hallamshire Hospital
Sheffield
UK
Disclosures
CE has received reimbursement for attending several conferences as well as lecture fees from Actelion Pharmaceuticals, GSK, and Bayer.
Maria Giovanna Triveri, MD, PhD
Assistant Professor of Cardiology
Medical Director of the Pulmonary Hypertension Program
Icahn School of Medicine at Mount Sinai Hospital
New York
NY
Disclosures
MGT has participated on Advisory Boards of Bayer and Actelion and received financial compensation for attendance.
References
Key articles
Simonneau G, Montani D, Celermajer DS, et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J. 2019 Jan;53(1):1801913.Full text Abstract
Humbert M, Kovacs G, Hoeper MM, et al; ESC/ERS Scientific Document Group. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022 Oct 11;43(38):3618-731. [Erratum in: Eur Heart J. 2023 Feb 23:ehad005.]Full text Abstract
Rich S, Dantzker DR, Ayres SM, et al. Primary pulmonary hypertension. A national prospective study. Ann Intern Med. 1987 Aug;107(2):216-23. Abstract
Klinger JR, Elliott CG, Levine DJ, et al. Therapy for pulmonary arterial hypertension in adults: update of the CHEST guideline and expert panel report. Chest. 2019 Mar;155(3):565-86.[Erratum in: Chest. 2021 Jan;159(1):457.] Abstract
Frost A, Badesch D, Gibbs JSR, et al. Diagnosis of pulmonary hypertension. Eur Respir J. 2019 Jan;53(1):1801904.Full text Abstract
Galiè N, Channick RN, Frantz RP, et al. Risk stratification and medical therapy of pulmonary arterial hypertension. Eur Respir J. 2019 Jan;53(1):1801889.Full text Abstract
Reference articles
A full list of sources referenced in this topic is available to users with access to all of BMJ Best Practice.
Differentials
- Hipertensão arterial pulmonar (HAP) associada a cardiopatia esquerda (hipertensão venosa pulmonar)
- HAP associada a distúrbios respiratórios e/ou hipóxia
- HAP decorrente de doença trombótica e/ou embólica crônica
More DifferentialsGuidelines
- Pulmonary rehabilitation for adults with chronic respiratory disease
- ACR appropriateness criteria® suspected pulmonary hypertension
More Guidelines Log in or subscribe to access all of BMJ Best Practice
Log in or subscribe to access all of BMJ Best Practice
Use of this content is subject to our disclaimer