Resumo
Definição
História e exame físico
Principais fatores diagnósticos
- presença de fatores de risco
- erupção cutânea polimorfa
- hiperemia conjuntival
- mucosite
- alterações cutâneas nos membros periféricos
- linfonodos cervicais aumentados
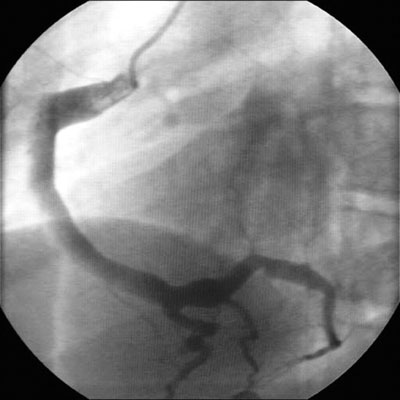
- aneurismas da artéria coronária
- febre e irritabilidade extrema
Outros fatores diagnósticos
- pericardite com efusão
- insuficiência cardíaca congestiva
- dor na articulação ou edema
- rouquidão
- manifestações neurológicas
- manifestações gastrointestinais
- manifestações urológicas
- outras manifestações dermatológicas
Fatores de risco
- ascendência asiática
- 3 meses a 4 anos de idade
- sexo masculino
Investigações diagnósticas
Primeiras investigações a serem solicitadas
- Hemograma completo
- velocidade de hemossedimentação (VHS)
- proteína C-reativa sérica
- ecocardiograma
- testes séricos da função hepática
- urinálise
- eletrocardiograma
Investigações a serem consideradas
- radiografia torácica
- ultrassonografia da vesícula biliar
- ultrassonografia dos testículos
- punção lombar
- angiografia por tomografia computadorizada
- angiografia por ressonância magnética (ARM)
- cateterismo cardíaco e angiografia
Novos exames
- testes de peptídeos natriuréticos
Algoritmo de tratamento
apresentação ≤10 dias a partir do início; ou apresentação >10 dias do início com evidências de inflamação contínua
apresentação >10 dias do início sem evidências de inflamação contínua
após o episódio inicial: Z-score sempre <2; sem comprometimento em nenhum momento
após o episódio inicial: Z-score ≥2.0 a <2.5; apenas dilatação
após episódio inicial: Z-score ≥2.5 a <5.0; aneurisma pequeno
após o episódio inicial: Z-score ≥5 a <10 (com dimensão luminal absoluta <8 mm); aneurisma médio
após episódio inicial: Z-score ≥10 ou diâmetro luminal absoluto ≥8 mm; aneurisma grande ou gigante
Colaboradores
Autores
Paul Brogan, BSc(Hon), MBChB(Hon), FRCPCH, MSc, PhD
Professor of vasculitis
University College London
London
UK
Declarações
PB is chief investigator of the KDCAAP trial, results pending; trustee of Societi, a patient KD organisation; and is an author of several references cited in this topic.
Kirsty McLellan, BMedSci, MBChB, MRCPCH
Specialist Registrar in Paediatric Rheumatology
Great Ormond Street Hospital
London
UK
Declarações
KM declares she has no competing interests.
Agradecimentos
Dr Paul Brogan and Dr Kirsty McLellan would like to gratefully acknowledge Professor Abraham Gedalia and Dr James Krulisky, previous contributors to this topic.
Declarações
AG declares that he has no competing interests. JK declares that he is a paid consultant for Axia Medical Solutions, a small skincare company from Carlsbad, CA.
Revisores
Michael Levin, null
Professor of International Child Health
Imperial College London
London
Declarações
ML declares that he has no competing interests.
Kirsten Bourke Dummer, MD
Clinical Professor, Pediatrics
Division of Pediatric Cardiology
UC San Diego/Rady Children’s Hospital
San Diego
CA
Declarações
KBD declares that she has no competing interests.
David Burgner, BSc(Hons), MBChB, MRCP, MRCPCH, FRACP, DTMH, PhD
Principal Research Fellow
Murdoch Childrens Research Institute
The Royal Children’s Hospital
Victoria
Australia
Declarações
DB has received competitive research funding from the National Heart Foundation Australia and from the Agency for Science, Technology and Research of the Singapore Government. He is co-inventor on a patent related to diagnostics submitted through the Genome Institute of Singapore.
Créditos aos pareceristas
Os tópicos do BMJ Best Practice são constantemente atualizados, seguindo os desenvolvimentos das evidências e das diretrizes. Os pareceristas aqui listados revisaram o conteúdo pelo menos uma vez durante a história do tópico.
Declarações
As afiliações e declarações dos pareceristas referem--se ao momento da revisão.
Referências
Principais artigos
McCrindle BW, Rowley AH, Newburger JW, et al; American Heart Association. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017 Apr 25;135(17):e927-99.Texto completo Resumo
de Graeff N, Groot N, Ozen S, et al. European consensus-based recommendations for the diagnosis and treatment of Kawasaki disease - the SHARE initiative. Rheumatology (Oxford). 2019 Apr 1;58(4):672-82.Texto completo Resumo
Jone PN, Tremoulet A, Choueiter N, et al. Update on diagnosis and management of Kawasaki disease: a scientific statement from the American Heart Association. Circulation. 2024 Dec 3;150(23):e481-500.Texto completo Resumo
Gorelik M, Chung SA, Ardalan K, et al. 2021 American College of Rheumatology/Vasculitis Foundation guideline for the management of Kawasaki disease. Arthritis Care Res (Hoboken). 2022 Apr;74(4):538-48. Resumo
Artigos de referência
Uma lista completa das fontes referenciadas neste tópico está disponível para os usuários com acesso total ao BMJ Best Practice.
Diagnósticos diferenciais
- Infecção por estafilococos ou estreptococos
- Artrite idiopática juvenil sistêmica
- Escarlatina
Mais Diagnósticos diferenciaisDiretrizes
- Update on diagnosis and management of Kawasaki disease: a scientific statement from the American Heart Association
- European consensus-based recommendations for the diagnosis and treatment of Kawasaki disease - the SHARE initiative
Mais Diretrizes Conectar-se ou assinar para acessar todo o BMJ Best Practice
Conectar-se ou assinar para acessar todo o BMJ Best Practice
O uso deste conteúdo está sujeito ao nosso aviso legal