შეჯამება
განსაზღვრება
ანამნეზი და გასინჯვა
ძირითადი დიაგნოსტიკური ფაქტორები
- დიარეა, განსაკუთრებით სისხლიანი დიარეა
- ბავშვებში, განსაკუთრებით 5 წლამდე ასაკის პაციენტებში
სხვა დიაგნოსტიკური ფაქტორები
- შიგა ტოქსინის წარმომქმნელი E coli დადასტურებული არაჰოსპიტალური ეპიდაფეთქება
- ანამნეზში ისეთი საკვების მიღება, რომელიც შესაძლოა დაბინძურებული ყოფილიყო შიგა ტოქსინწარმომქმნელი E coli-ით.
- უჩვეულო გვერდითი მოვლენები, რომლებიც მოჰყვება მკურნალობას ციკლოსპორინით, ზოგიერთი ქიმიოთერაპიული აგენტით, კიბოს მიზნობრივად მოქმედი აგენტებით და ქინინით
- ორსულობა ან მშობიარობის შემდგომი მდგომარეობა
- უჩვეული გვერდითი მოვლენა, რომელიც ვლინდება ძვლის ტვინის გადანერგვის შემდგომ
- ჰემოლიზურ-ურემიული სინდრომის მსგავსი სინდრომის შესაძლო ოჯახური ანამნეზი
რისკფაქტორები
- დაბინძურებული საკვების ან წყლის მიღება
- ტოქსოგენური E coli არაჰოსპიტალური ეპიდაფეთქება
- ინფიცირებულ პირებთან ექსპოზიცია ინსტიტუციონალურ პირობებში
- გენეტიკური წინასწარგანწყობა (ატიპური HUS)
- ძვლის ტვინის ტრანსპლანტანტი
- ციკლოსპორინთან, ზოგიერთ ქიმიოთერაპიულ აგენტთან, კიბოს ტარგეტულ აგენტებთან და ქინინთან ექსპოზიცია
- ორსულობასთან ან მშობიარობის შემდგომ პერიოდთან დაკავშირებული
დიაგნოსტიკური კვლევები
1-ად შესაკვეთი გამოკვლევები
- FBC
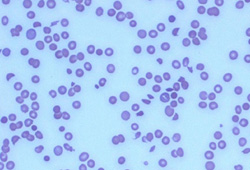
- პერიფერიული სისხლის ნაცხში
- თირკმლის ფუნქცია/კრეატინინი
- შრატის ელექტროლიტები (ნატრიუმი, კალიუმი, ქლორიდი და ბიკარბონატი, კალციუმი და ფოსფორი)
- პროთრომბინის დრო, თრომბოპლასტინის პარციალური დრო
- ლაქტატ დეჰიდროგენაზა (LDH)
- ჰაპტოგლობინი
- განავლის კულტურა სორბიტოლ-MacConkey აგარზე შიგა ტოქსინწარმომქმნელი Escherichia coli დეტექციისთის
- პოლიმერაზული ჯაჭვის რეაქცია (PCR) Shiga ტოქსინის 1 / Shiga ტოქსინის 2 გამოვლენის მიზნით
- ცილები, რომლებიც მონაწილეობას იღებენ კომპლემენტის რეგულაციაში
გასათვალისწინებელი კვლევები
- შარდის საერთო ანალიზი
- ADAMTS13-ის დონე
- ღვიძლის ფუნქციური სინჯები
- შრატის ამილაზა, ლიპაზა, გლუკოზა
მკურნალობის ალგორითმი
შიგა ტოქსინ-წარმომქმნელი Escherichia coli (STEC) HUS
ატიპური HUS
მეორადი HUS: არა Streptococcus pneumoniae გამო
მეორადი HUS: S pneumoniae გამო
კონტრიბუტორები
ავტორები
Sharon Andreoli, MD
Byron P. and Francis D. Hollet Professor of Pediatrics, Pediatric Nephrology
Indiana University School of Medicine
Indianapolis
IN
გაფრთხილება:
SA owns stock in Merck and Pfizer, and has been a consultant for Reata Pharmaceuticals. SA is on the Editorial Board of Pediatric Nephrology and the Journal of Pediatrics.
Myda Khalid, MD
Associate Professor of Pediatric Nephrology
Indiana University School of Medicine
Indianapolis
IN
გაფრთხილება:
MK declares that she has no competing interests.
მადლიერება
Dr Sharon Andreoli and Dr Myda Khalid would like to gratefully acknowledge Dr Ann Zimrin and Dr John Hess, previous contributors to this topic.
გაფრთხილება:
AZ and JH declare that they have no competing interests.
რეცენზენტები
Rebecca Connor, MD
Chief Fellow
Section of Hematology and Oncology
Department of Internal Medicine
Wake Forest University Baptist Medical Center
Winston-Salem
NC
გაფრთხილება:
RC declares that she has no competing interests.
რეცენზენტების განცხადებები
BMJ Best Practice-ის თემების განახლება სხვადასხვა პერიოდულობით ხდება მტკიცებულებებისა და რეკომენდაციების განვითარების შესაბამისად. ქვემოთ ჩამოთვლილმა რეცენზენტებმა თემის არსებობის მანძილზე კონტენტს ერთხელ მაინც გადახედეს.
გაფრთხილება
რეცენზენტების აფილიაციები და გაფრთხილებები მოცემულია გადახედვის მომენტისთვის.
წყაროები
ძირითადი სტატიები
Fakhouri F, Zuber J, Frémeaux-Bacchi V, et al. Haemolytic uraemic syndrome. Lancet. 2017 Aug 12;390(10095):681-96. აბსტრაქტი
Banatvala N, Griffin PM, Greene KD, et al. The United States national prospective hemolytic uremic syndrome study: microbiologic, serologic, clinical and epidemiologic findings. J Infect Dis. 2001 Apr 1;183(7):1063-70. აბსტრაქტი
Tarr PI, Gordon CA, Chandler WL. Shiga-toxin-producing Escherichia coli and haemolytic uraemic syndrome. Lancet. 2005 Mar 19-25;365(9464):1073-86. აბსტრაქტი
Wong CS, Jelacic S, Habeeb RL, et al. The risk of the hemolytic-uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections. N Engl J Med. 2000 Jun 29;342(26):1930-6.სრული ტექსტი აბსტრაქტი
McKee RS, Schnadower D, Tarr PI, et al; Pediatric Emergency Medicine Collaborative Research Committee and Pediatric Emergency Research Canada. Predicting hemolytic uremic syndrome and renal replacement therapy in Shiga toxin-producing Escherichia coli-infected children. Clin Infect Dis. 2020 Apr 10;70(8):1643-51.სრული ტექსტი აბსტრაქტი
Boyce TG, Swerdlow DL, Griffin PM. Escherichia coli O157:H7 and the hemolytic uremic syndrome. N Engl J Med. 1995 Aug 10;333(6):364-8. აბსტრაქტი
Rathbone J, Kaltenthaler E, Richards A, et al. A systematic review of eculizumab for atypical haemolytic uraemic syndrome (aHUS). BMJ Open. 2013 Nov 4;3(11):e003573.სრული ტექსტი აბსტრაქტი
Loirat C, Fakhouri F, Ariceta G, et al. An international consensus approach to the management of atypical hemolytic uremic syndrome in children. Pediatr Nephrol. 2016 Jan;31(1):15-39. აბსტრაქტი
გამოყენებული სტატიები
ამ თემაში მოხსენიებული წყაროების სრული სია ხელმისაწვდომია მომხმარებლებისთვის, რომლებსაც აქვთ წვდომა BMJ Best Practice-ის ყველა ნაწილზე.
დიფერენციული დიაგნოზები
- თრომბოზული თრომბოციტოპენიური პურპურა
- ავთვისებიანი არტერიალური ჰიპერტენზია
- სისტემური წითელი მგლურა (SLE)
მეტი დიფერენციული დიაგნოზებიგაიდლაინები
- Guidelines on hemolytic uremic syndrome by Indian Society of Pediatric Nephrology: key messages
- Hemolytic uremic syndrome in a developing country: consensus guidelines
მეტი გაიდლაინები შედით სისტემაში ან გამოიწერეთ BMJ Best Practice
შედით სისტემაში ან გამოიწერეთ BMJ Best Practice
ამ მასალის გამოყენება ექვემდებარება ჩვენს განცხადებას