Summary
Definition
History and exam
Key diagnostic factors
- pallor
- jaundice
Other diagnostic factors
- fatigue
- shortness of breath
- dizziness
- splenomegaly
- active infections
- episodic dark urine (hemoglobinuria)
- triggered by exposure to cold
Risk factors
- autoimmune disorders
- lymphoproliferative disorders
- prosthetic heart valve
- family origin in Mediterranean, Middle East, Africa, or Southeast Asia
- family history of hemoglobinopathy or red blood cell membrane defects
- paroxysmal nocturnal hemoglobinuria
- recent exposure to cephalosporins, penicillins, quinine derivatives, or nonsteroidal anti-inflammatory drugs
- recent exposure to naphthalene or fava beans
- thermal injury
- exceptional exertion
- recent exposure to nitrites, dapsone, ribavirin, or phenazopyridine
- recent paraquat ingestion
- malaria
- babesiosis
- bartonellosis
- leishmaniasis
- Clostridium perfringens infection
- Haemophilus influenzae type B infection
- liver disease
Diagnostic tests
1st tests to order
- CBC
- MCHC
- reticulocyte count
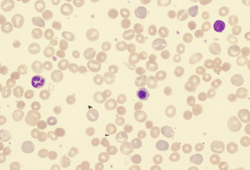
- peripheral smear
- unconjugated (indirect) bilirubin
- LDH
- haptoglobin
- urinalysis
Tests to consider
- direct antiglobulin test (Coombs)
- creatinine, BUN
- LFTs
- Donath-Landsteiner antibody
- Hb electrophoresis
- flow cytometry for CD55/CD59
- glucose-6-phosphate dehydrogenase (G6PD) fluorescent spot test and spectrophotometry
- antinuclear antibody
Treatment algorithm
acquired: direct antiglobulin test (Coombs) positive
acquired: direct antiglobulin test (Coombs) negative
inherited disorders
Contributors
Authors
John Densmore, MD, PhD
Associate Professor of Clinical Medicine
Department of Medicine
University of Virginia
Charlottesville
VA
Disclosures
JD declares that he has no competing interests.
Acknowledgements
Dr John Densmore would like to gratefully acknowledge Dr Michelle Loch, a previous contributor to this monograph. ML declares that she has no competing interests.
Peer reviewers
Pasquale Niscola, MD
Hematology Unit
Sant'Eugenio Hospital
Rome
Italy
Disclosures
PN declares that he has no competing interests.
Alan Lichtin, MD
Staff Hematologist-Oncologist
Hematologic Oncology and Blood Disorders
Cleveland Clinic
Associate Professor
Internal Medicine
Cleveland Clinic Lerner College of Medicine
Cleveland
OH
Disclosures
AL declares that he has no competing interests.
Peer reviewer acknowledgements
BMJ Best Practice topics are updated on a rolling basis in line with developments in evidence and guidance. The peer reviewers listed here have reviewed the content at least once during the history of the topic.
Disclosures
Peer reviewer affiliations and disclosures pertain to the time of the review.
References
Key articles
Go RS, Winters JL, Kay NE. How I treat autoimmune hemolytic anemia. Blood. 2017 Jun 1;129(22):2971-9 Abstract
Hill QA, Stamps R, Massey E, et al. The diagnosis and management of primary autoimmune haemolytic anaemia. Br J Haematol. 2017 Feb;176(3):395-411.Full text Abstract
Hill QA, Stamps R, Massey E, et al. Guidelines on the management of drug-induced immune and secondary autoimmune, haemolytic anaemia. Br J Haematol. 2017 Apr;177(2):208-20.Full text Abstract
Reference articles
A full list of sources referenced in this topic is available to users with access to all of BMJ Best Practice.
Differentials
- Anemia due to blood loss
- Underproduction anemia
- Transfusion reaction
More DifferentialsGuidelines
- Diagnosis and treatment of autoimmune hemolytic anemia in adults
- Recommendations regarding splenectomy in hereditary hemolytic anemias
More GuidelinesVideos
Venepuncture and phlebotomy: animated demonstration
Peripheral intravascular catheter: animated demonstration
More videos Log in or subscribe to access all of BMJ Best Practice
Log in or subscribe to access all of BMJ Best Practice
Use of this content is subject to our disclaimer