Summary
Anemia is a hemoglobin (Hb) level two standard deviations below the mean for the age and sex of the patient. Reference ranges vary between laboratories. The World Health Organization (WHO) recommends the following hemoglobin cutoffs to define anemia in the individual:[1]
Hb <10.5 g/dL in children ages 6 to 23 months
Hb <11 g/dL in children ages 24 to 59 months
Hb <11.5 g/dL children ages 5 to 11 years
Hb <12 g/dL in children ages 12 to 14 years
Hb <12 g/dL in nonpregnant adult females (ages 15 years and over)
Hb <13 g/dL in adult males (ages 15 years and over)
Hb <11 g/dL during the first trimester pregnancy
Hb <10.5 g/dL during the second trimester pregnancy
Hb <11 g/dL during the third trimester pregnancy
Adjustments to hemoglobin cut-off values may be required, according to external factors, such as cigarette smoking and the population’s elevation above sea level.[1]
Anemia is commonly seen in general medical practice.[2][3] Risk factors include extremes of age, female sex, lactation, and pregnancy. The most common cause of anemia globally is dietary iron deficiency.[4][5]
Anemia can cause significant morbidity if left untreated, and is often the presenting sign of a more serious underlying condition.[6] The rate at which anemia develops is often as important as the severity, as a rapid decline can overwhelm the compensatory mechanisms of the body.
For all population groups combined, the Global Burden of Disease Study (2021) estimated that approximately 24% of the world’s population had some form of anemia, affecting 1.9 billion people.[5] Sub-Saharan Africa and South Asia are particularly affected.[5]
The WHO estimated that 30.7% of women of reproductive age were anemic in 2023, with the highest prevalence in South-East Asia and Africa.[7]
Globally, in 2019, 40% of children ages 6-59 months were anemic.[8]
Pathophysiology
Erythropoiesis takes place within the bone marrow and is controlled by the stromal network, cytokines, and the hormone erythropoietin. Through a series of differentiation steps, hematopoietic stem cells become reticulocytes (red blood cells [RBCs] with an intact ribosomal network).
Reticulocytes remain in the bone marrow for 3 days before being released into the circulation. After approximately one day in the circulation, reticulocytes lose their ribosomal network and become mature RBCs, which circulate for 110-120 days before being removed from the circulation by macrophages.[9]
Anemia develops when the rate of RBC production decreases and/or the rate of RBC loss increases.
Morphological classification of anemia
The most clinically useful classification system is based on the mean corpuscular volume (MCV).[3]
Microcytic (MCV <80 femtoliters [fL]).[Figure caption and citation for the preceding image starts]: Microcytic anemiaFrom the collection of Dr Robert Zaiden; used with permission [Citation ends].
Normocytic (MCV 80-100 femtoliters [fL]); can be hyperproliferative or hypoproliferative.
Hyperproliferative (reticulocyte count >2%): the proportion of circulating reticulocytes increases as part of a compensatory response to increased destruction or loss of RBCs. The cause is usually acute blood loss or hemolysis.
Hypoproliferative (reticulocyte count <2%): primarily disorders of decreased RBC production, and the proportion of circulating reticulocytes remains unchanged.
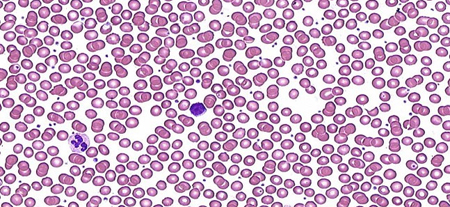
Macrocytic (MCV >100 femtoliters [fL]); can be megaloblastic or nonmegaloblastic.
Megaloblastic: a deficiency of DNA production or maturation resulting in the appearance of large immature RBCs (megaloblasts) and hypersegmented neutrophils in the circulation.
Nonmegaloblastic: encompasses all other causes of macrocytic anemia in which DNA synthesis is normal. Megaloblasts and hypersegmented neutrophils are absent.[Figure caption and citation for the preceding image starts]: Megaloblastic macrocytic anemiaFrom the collection of Dr Robert Zaiden; used with permission [Citation ends].
 [Figure caption and citation for the preceding image starts]: Classification of anemia: MCV, mean corpuscular volume; fL, femtolitersCreated by the BMJ Knowledge Centre [Citation ends].
[Figure caption and citation for the preceding image starts]: Classification of anemia: MCV, mean corpuscular volume; fL, femtolitersCreated by the BMJ Knowledge Centre [Citation ends].
Differentials
Common
- Trauma
- Acute gastrointestinal bleeding
- Surgery
- Menorrhagia
- Iron deficiency
- Vitamin B12 deficiency
- Folate deficiency
- Myelodysplastic syndrome
- Acute lymphoblastic leukemia
- Acute myeloid leukemia
- Chronic myeloid leukemia
- Hairy cell leukemia
- Acquired aplastic anemia
- Infiltration by secondary malignancy
- Pure red cell aplasia
- Drug toxicity
- Anemia of chronic disease
- Chronic kidney disease
- Chronic liver disease
- Pregnancy
Uncommon
- Rupture of a vascular aneurysm
- Generalized malnutrition
- Cytotoxic chemotherapy
- Radiation therapy
- Alcohol misuse
- Lead toxicity
- Hypothyroidism
- Autoimmune hemolytic anemia
- Transfusion reaction
- Malaria
- Viral hepatitis
- Toxoplasmosis
- Leishmaniasis
- Parvovirus B19 infection
- Infectious mononucleosis
- Cytomegalovirus (CMV)
- Sickle cell anemia
- Thalassemias
- Hereditary spherocytosis
- Glucose-6-phosphate dehydrogenase deficiency (G6PD)
- Bone marrow failure syndromes
- Hemolytic uremic syndrome
- Disseminated intravascular coagulation (DIC)
- Thrombotic thrombocytopenic purpura
- Hemangioma
- Malignant hypertension
- Prosthetic valves and surfaces
- Cutaneous burns
Contributors
Authors
Robert Zaiden, MD
Hematologist Oncologist
Baptist MD Anderson Cancer Center
Jacksonville
FL
Disclosures
RZ declares that he has received occasional honoraria from Aptitude Health, a marketing firm, for insight into treatment trends on gastrointestinal and genitourinary cancers (nothing related to the topic).
Acknowledgements
Dr Robert Zaiden would like to gratefully acknowledge Dr Fauzia Rana, a previous contributor to this topic.
Disclosures
FR declares that she has no competing interests.
Peer reviewers
Christoph Pechlaner, MD
Associate Professor of Medicine
Innsbruck Medical University
Innsbruck
Austria
Disclosures
CP declares that he has no competing interests.
John Densmore, MD, PhD
Associate Professor of Clinical Medicine
Department of Medicine
Division of Hematology/Oncology
University of Virginia
Charlottesville
VA
Disclosures
JD declares that he has no competing interests.
Carlos Aravena, MD
Internal Medicine Instructor
Member of Evidence Based Medicine Unit
Catholic University of Chile
Santiago
Chile
Disclosures
CA declares that he has no competing interests.
Peer reviewer acknowledgements
BMJ Best Practice topics are updated on a rolling basis in line with developments in evidence and guidance. The peer reviewers listed here have reviewed the content at least once during the history of the topic.
Disclosures
Peer reviewer affiliations and disclosures pertain to the time of the review.
References
Key articles
Snook J, Bhala N, Beales ILP, et al. British Society of Gastroenterology guidelines for the management of iron deficiency anaemia in adults. Gut. 2021 Nov;70(11):2030-51.Full text Abstract
Ko CW, Siddique SM, Patel A, et al. AGA clinical practice guidelines on the gastrointestinal evaluation of iron deficiency anemia. Gastroenterology. 2020 Sep;159(3):1085-94.Full text Abstract
Kulasekararaj A, Cavenagh J, Dokal I, et al. Guidelines for the diagnosis and management of adult aplastic anaemia: a British Society for Haematology guideline. Br J Haematol. 2024 Mar;204(3):784-804.Full text Abstract
Bain BJ, Daniel Y, Henthorn J, et al. Significant haemoglobinopathies: a guideline for screening and diagnosis. Br J Haematol. 2023 Jun;201(6):1047-65.Full text Abstract
Reference articles
A full list of sources referenced in this topic is available to users with access to all of BMJ Best Practice.
Patient information
Anemia, iron deficiency
More Patient informationVideos
Venepuncture and phlebotomy: animated demonstration
More videos Log in or subscribe to access all of BMJ Best Practice
Log in or subscribe to access all of BMJ Best Practice
Use of this content is subject to our disclaimer