Summary
Definition
HCL is an indolent mature B-cell neoplasm. It is considered to be a type of non-Hodgkin lymphoma. Seen under the microscope, the leukemic cells have delicate cytoplasmic projections resembling hair ("hairy cells"). HCL has a characteristic presentation of pancytopenia, splenomegaly, and hairy cells in the peripheral blood, bone marrow, and other hematopoietic organs.[Figure caption and citation for the preceding image starts]: Cytospin prepared from bone marrow aspirate illustrates the typical cell cytology, with oval- to bean-shaped nuclei and moderate amounts of cytoplasm with irregular cytoplasmic borders (Wright Giemsa 100×oil)From the collection of Lynn Moscinski, MD [Citation ends].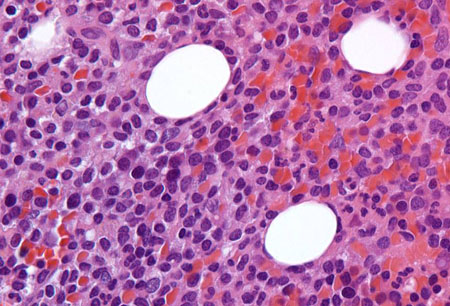 [Figure caption and citation for the preceding image starts]: Sections of core biopsy demonstrate lymphocytes with obvious cytoplasm within the marrow interstitium, associated with dilation of marrow sinuses and red blood cell collections (H&E 50×oil)From the collection of Lynn Moscinski, MD [Citation ends].
[Figure caption and citation for the preceding image starts]: Sections of core biopsy demonstrate lymphocytes with obvious cytoplasm within the marrow interstitium, associated with dilation of marrow sinuses and red blood cell collections (H&E 50×oil)From the collection of Lynn Moscinski, MD [Citation ends].
History and exam
Key diagnostic factors
- abdominal fullness or discomfort
- splenomegaly
Other diagnostic factors
- weakness and fatigue
- unexplained weight loss
- bruising and bleeding
- pallor
- recurrent infections
- hepatomegaly
- lymphadenopathy
- neurologic findings
- associated systemic immunologic disorders
Risk factors
- middle age
- male sex
- white ancestry
- western hemisphere location
- environmental exposures
- genetic predisposition
- Epstein-Barr virus
- infectious mononucleosis
Diagnostic tests
1st tests to order
- CBC with differential
- peripheral blood smear
- bone marrow trephine biopsy and aspiration (morphology assessment)
- immunophenotyping (immunohistochemistry or flow cytometry)
- comprehensive metabolic panel
- serum lactate dehydrogenase (LDH)
- viral serology for hepatitis B and C
Tests to consider
- molecular analysis (for BRAF V600E mutation or IGHV4-34 rearrangement)
- CT chest, abdomen, and pelvis
Treatment algorithm
no indication(s) for treatment
indication(s) for treatment present: without splenic rupture or massive splenomegaly or marked thrombocytopenia precluding chemotherapy
indication(s) for treatment present: with massive symptomatic splenomegaly or splenic rupture or marked thrombocytopenia precluding chemotherapy
early relapse (<2 years) or refractory disease
late relapse (≥2 years)
Contributors
Authors
Ambuj Kumar, MD, MPH
Professor
USF Health Office of Research
Department of Internal Medicine, College of Medicine
Moffitt Cancer Center & Research Institute, Department of Health Outcomes & Behavior
University of South Florida
Tampa
FL
Disclosures
AK declares that he has no competing interests.
Mohamed A. Kharfan-Dabaja, MD, MBA, FACP
Professor
Division of Hematology-Oncology
Blood and Marrow Transplantation Program
Mayo Clinic
Jacksonville
FL
Disclosures
MKD declares that he has no competing interests.
Acknowledgements
Dr Ambuj Kumar and Dr Mohamed Kharfan-Dabaja would like to gratefully acknowledge Dr Benjamin Djulbegovic, a previous contributor to this topic.
Disclosures
BD declares that he has no competing interests.
Peer reviewers
Roger Lyons, MD
Clinical Professor of Medicine
University of Texas Health Science Center San Antonio
San Antonio
TX
Disclosures
RL declares that he has no competing interests.
Rebecca Connor, MD
Chief Fellow
Section of Hematology and Oncology
Department of Internal Medicine
Wake Forest University Baptist Medical Center
Winston-Salem
NC
Disclosures
RC declares that she has no competing interests.
Claire Dearden, BSc, MD, FRCP, FRCPath
Consultant Haematologist
The Royal Marsden Hospital
Sutton
Surrey
UK
Disclosures
CD declares that she has no competing interests.
Peer reviewer acknowledgements
BMJ Best Practice topics are updated on a rolling basis in line with developments in evidence and guidance. The peer reviewers listed here have reviewed the content at least once during the history of the topic.
Disclosures
Peer reviewer affiliations and disclosures pertain to the time of the review.
References
Key articles
Parry-Jones N, Joshi A, Forconi F, et al. Guideline for diagnosis and management of hairy cell leukaemia (HCL) and hairy cell variant (HCL-V). Br J Haematol. 2020 Dec;191(5):730-7.Full text Abstract
Troussard X, Maître E, Paillassa J. Hairy cell leukemia 2024: update on diagnosis, risk-stratification, and treatment - annual updates in hematological malignancies. Am J Hematol. 2024 Apr;99(4):679-96.Full text Abstract
Grever MR, Abdel-Wahab O, Andritsos LA, et al. Consensus guidelines for the diagnosis and management of patients with classic hairy cell leukemia. Blood. 2017 Feb 2;129(5):553-60.Full text Abstract
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: hairy cell leukemia [internet publication].Full text
Robak T, Matutes E, Catovsky D, et al. Hairy cell leukaemia: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015 Sep;26(suppl 5):v100-7.Full text Abstract
Reference articles
A full list of sources referenced in this topic is available to users with access to all of BMJ Best Practice.
Differentials
- Chronic lymphocytic leukemia (CLL)
- Mantle cell lymphoma
- Prolymphocytic leukemia
More DifferentialsGuidelines
- ACR Appropriateness Criteria staging and follow-up of leukemia
- NCCN clinical practice guidelines in oncology: hairy cell leukemia
More Guidelines Log in or subscribe to access all of BMJ Best Practice
Log in or subscribe to access all of BMJ Best Practice
Use of this content is subject to our disclaimer