Summary
Definition
MALT lymphoma (also known as extranodal marginal zone lymphoma [EMZL] of MALT) is a mature B-cell non-Hodgkin lymphoma.[1][2] It is a marginal zone lymphoma (MZL).[3]
Other MZLs include splenic MZL (SMZL) and nodal MZL (NMZL). See Non-Hodgkin lymphoma for more information on SMZL and NMZL.
MALT lymphoma develops at extranodal sites. The stomach is the most commonly affected site (known as gastric MALT lymphoma), but any extranodal site can be affected.[4][5][6]
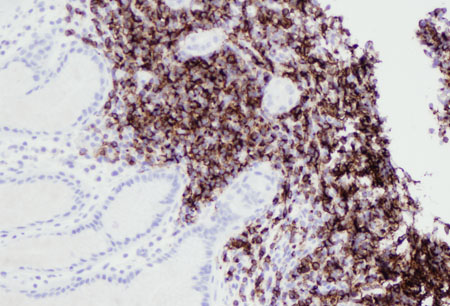
MALT lymphomas are composed of morphologically heterogenous small B cells, including marginal zone cells, cells resembling monocytoid cells, small lymphocytes, and scattered immunoblasts and centroblast-like cells.[7] Plasmacytic differentiation occurs in some patients. Neoplastic cells are located in the marginal zone of reactive B-cell follicles and extend into the interfollicular region. Lymphoepithelial lesions develop in epithelial tissues due to infiltration of the epithelium with neoplastic cells.[7]
[Figure caption and citation for the preceding image starts]: MALT lymphoma has a polymorphous lymphoid infiltrate that can include small lymphocytes, monocytoid B cells, centrocyte-like cells and cells with plasmacytoid differentiation. Scattered immunoblasts and centroblast-like cells may also be seenHollie N, et al. J Clin Pathol. 2020; 73: 378-83; used with permission [Citation ends].
History and exam
Key diagnostic factors
- history of Helicobacter pylori gastritis
- history of autoimmune disorder
- age >60 years
- dyspepsia
- epigastric discomfort
- skin lesions
- red eye ± photophobia
- conjunctival fornix mass
- painless proptosis, motility disturbances of the eye, diplopia, ptosis, decreased vision
Other diagnostic factors
- abdominal pain, nausea, diarrhea, malabsorption, vomiting
- GI bleeding, perforation, and obstruction
- fever
- night sweats
- weight loss
- shortness of breath, hemoptysis, cough
- salivary gland swelling
- thyroid swelling
- esophageal/tracheal obstruction (shortness of breath, dysphagia, tracheal deviation)
- breast lump
- focal neurologic deficits
- lymphadenopathy
Risk factors
- Helicobacter pylori infection
- age >60 years
- autoimmune disease
- Chlamydia psittaci infection
- Campylobacter jejuni infection
- Borrelia burgdorferi infection
- hepatitis C virus infection
- hepatitis B virus infection
- HIV infection
- achromobacter xylosoxidans infection
Diagnostic tests
1st tests to order
- CBC with differential
- blood smear
- comprehensive metabolic panel (including LFTs)
- serum lactate dehydrogenase (LDH)
- serum beta-2 microglobulin
- upper GI endoscopy
- tissue biopsy of affected site
- immunophenotyping
- H pylori (histologic testing)
- CT scan
Tests to consider
- H pylori (stool antigen test)
- H pylori (urea breath test)
- H pylori (serology test)
- PCR testing for infectious agents
- bone marrow biopsy with aspirate
- genetic studies
- immunoglobulin gene rearrangement studies
- MYD88 mutation testing
- serum protein electrophoresis
- 18F-fluorodeoxyglucose (FDG) PET/CT scan
- endoscopic ultrasound of the stomach
- lower GI endoscopy
- MRI orbit, brain
- mammography
- breast ultrasound
- MRI breast
- thyroid ultrasound
- bronchoscopy
- hepatitis C serology
- hepatitis B serology
- HIV serology
- multigated acquisition (MUGA) scan
- echocardiography
Treatment algorithm
localized gastric MALT lymphoma: Helicobacter pylori-positive and t(11;18)-negative (or unknown)
localized gastric MALT lymphoma: Helicobacter pylori-negative, or Helicobacter pylori-positive and t(11;18)-positive
advanced gastric MALT lymphoma
localized nongastric MALT lymphoma
advanced nongastric MALT lymphoma
high-grade histologic transformation
Contributors
Authors
Christopher McNamara, MBBS (Hons), FRACP, FRCPA, FRCPath
Consultant Haematologist
Royal Free Hospital
London
UK
Disclosures
CM declares that he has no competing interests.
Acknowledgements
Dr Christopher McNamara wishes to gratefully acknowledge Dr Rahul Joshi, a previous contributor to this topic. RJ declared that he had no competing interests. Unfortunately, we have since been made aware that Dr Rahul Joshi is deceased.
Peer reviewers
Markus Raderer, MD
Professor of Medicine
Department of Internal Medicine I
Division of Oncology
Medical University Vienna
Austria
Disclosures
MR is an author of a number of references cited in this topic.
Alan Lichtin, MD
Staff Hematologist
Cleveland Clinic Taussig Cancer Center
Cleveland
OH
Disclosures
AL declares that he has no competing interests.
Ian Chau, MD
Consultant Medical Oncologist
Royal Marsden Hospital
Sutton
UK
Disclosures
IC has been reimbursed by Roche Products, the manufacturer of rituximab, for attending several conferences. IC has also served on advisory boards and received honorarium for giving presentations for Roche Products. IC has received research funding from Novartis to conduct academic studies in the treatment of colorectal cancer.
Peer reviewer acknowledgements
BMJ Best Practice topics are updated on a rolling basis in line with developments in evidence and guidance. The peer reviewers listed here have reviewed the content at least once during the history of the topic.
Disclosures
Peer reviewer affiliations and disclosures pertain to the time of the review.
References
Key articles
Walewska R, Eyre TA, Barrington S, et al. Guideline for the diagnosis and management of marginal zone lymphomas: a British Society of Haematology guideline. Br J Haematol. 2024 Jan;204(1):86-107.Full text Abstract
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: B-cell lymphomas [internet publication].Full text
Eyre TA, Cwynarski K, d'Amore F, et al. Lymphomas: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2025 Nov;36(11):1263-84.Full text Abstract
Reference articles
A full list of sources referenced in this topic is available to users with access to all of BMJ Best Practice.
Differentials
- Mantle cell lymphoma
- Chronic lymphocytic leukemia/small lymphocytic lymphoma
- Follicular lymphoma
More DifferentialsGuidelines
- NCCN clinical practice guidelines in oncology: B-cell lymphomas
- Lymphomas: ESMO clinical practice guideline for diagnosis, treatment and follow-up
More GuidelinesPatient information
Non-Hodgkin lymphoma
More Patient information Log in or subscribe to access all of BMJ Best Practice
Log in or subscribe to access all of BMJ Best Practice
Use of this content is subject to our disclaimer