Summary
Definition
Gynecomastia is the benign enlargement of the male breast glandular tissue with firm tissue extending concentrically beyond the nipple. Histologically, gynecomastia is the benign proliferation of breast ducts and duct epithelial hyperplasia accompanied by varying amounts of inflammation, edema, stroma, and fibrosis. Male breast enlargement entirely due to adipose tissue is called pseudogynecomastia.[Figure caption and citation for the preceding image starts]: Histology: gynecomastia; clusters of ducts, halos of edema, fibrous background; 5X magnificationFrom the collection of Catherine B. Niewoehner, MD [Citation ends].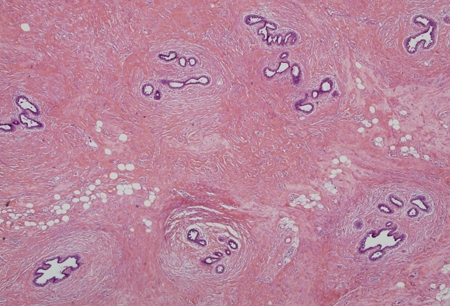
History and exam
Key diagnostic factors
- palpable breast tissue
- newborn age
- pubertal age
- older adult age
- accidental medication exposure in children
- substance use disorder
- acne in adult males
- obesity
- breast pain
- small or soft testicles
Other diagnostic factors
- erectile dysfunction or decreased libido
- nutritional supplements
- differences in sex development (DSD)
- delayed secondary sex characteristics
- precocious puberty
- weight loss and malnutrition
- signs or symptoms of hypothalamic or pituitary disease
- signs or symptoms of liver failure (e.g., jaundice, ascites, spiders)
- signs or symptoms of hyperthyroidism (e.g., heat intolerance, weight loss, goiter)
- decreased body hair
- painless or enlarging testicular mass
- diminished strength or muscle atrophy
Risk factors
- anabolic steroid usage
- prostate cancer
- hormone therapy for gender dysphoria
- drugs that reduce testosterone synthesis
- drugs that impair testosterone action
- drugs that increase estrogen levels or stimulate estrogen receptors
- occupational exposure to embalming fluid or oral contraceptives
- contact with environmental phytoestrogens or phthalates
- hyperthyroidism
- renal failure
- cirrhosis
- drugs with complex or unknown mechanisms
Diagnostic tests
1st tests to order
- serum TSH
- serum creatinine
- serum LFTs
Tests to consider
- serum total testosterone
- serum LH
- serum estradiol
- serum sex hormone binding globulin (SHBG)
- serum free testosterone
- serum beta hCG
- serum dehydroepiandrosterone-sulfate (DHEAS)
- serum prolactin
- mammogram
- core biopsy of breast (if cancer suspected)
- testicular ultrasound
- abdominal CT/MRI (if adrenal adenoma or carcinoma suspected)
Treatment algorithm
adults
pubertal idiopathic gynecomastia
infantile and prepubertal gynecomastia
Contributors
Authors
Glenn Braunstein, MD
Professor of Medicine
Cedars-Sinai Medical Center
Los Angeles
CA
Disclosures
GB writes the chapters on Gynecomastia for UpToDate and Encyclopedia of Endocrine Diseases. GB is an author of references cited in this topic.
Acknowledgements
Dr Glenn Braunstein would like to gratefully acknowledge Dr Catherine B. Niewoehner, a previous contributor to this topic.
Peer reviewers
Dennis Styne, MD
Professor of Pediatrics
Rumsey Chair of Pediatric Endocrinology
University of California
Sacramento
CA
Disclosures
DS declares that he has no competing interests.
Harold Carlson, MD
Professor of Medicine and Head of Endocrinology
Stony Brook University
Stony Brook
NY
Disclosures
HC is an author of a reference cited in this topic.
Peer reviewer acknowledgements
BMJ Best Practice topics are updated on a rolling basis in line with developments in evidence and guidance. The peer reviewers listed here have reviewed the content at least once during the history of the topic.
Disclosures
Peer reviewer affiliations and disclosures pertain to the time of the review.
References
Key articles
Kanakis GA, Nordkap L, Bang AK, et al. EAA clinical practice guidelines-gynecomastia evaluation and management. Andrology. 2019 Nov;7(6):778-93.Full text Abstract
Bromley HL, Dave R, Lord N, et al. Gynaecomastia: when and why to refer to specialist care. Br J Gen Pract. 2021 Apr;71(705):185-8.Full text Abstract
Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018 May 1;103(5):1715-44.Full text Abstract
American College of Radiology. ACR appropriateness criteria: evaluation of the symptomatic male breast. 2018 [internet publication].Full text
Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and management of testosterone deficiency: AUA guideline. J Urol. 2018 Aug;200(2):423-32.Full text Abstract
Reference articles
A full list of sources referenced in this topic is available to users with access to all of BMJ Best Practice.
Differentials
- Breast cancer
- Benign breast masses
- Pseudogynecomastia
More DifferentialsGuidelines
- EAU guidelines on sexual and reproductive health
- ACR appropriateness criteria: evaluation of nipple discharge
More GuidelinesPatient information
Obesity - drugs and surgery
More Patient information Log in or subscribe to access all of BMJ Best Practice
Log in or subscribe to access all of BMJ Best Practice
Use of this content is subject to our disclaimer