
Summary
Tachycardia, generally defined as a heart rate ≥100 bpm, can be a normal physiologic response to a systemic process or a manifestation of underlying pathology.[1][2] The normal heart rate varies with age. The normal sinus rate in infants is 110 to 150 bpm, which gradually slows with age.[3]
Classification of tachyarrhythmia
Several methods of classification are helpful in organizing and evaluating tachycardias. These include: sinus versus non-sinus causes; atrial versus ventricular arrhythmias; narrow- versus wide-complex tachycardias; regular versus irregular arrhythmias; and classification based on the site of origin of the arrhythmia.[1]
Sinus versus non-sinus causes
Sinus tachycardia is a common cause of tachycardia that can often be mistaken for an arrhythmia. Diagnosis depends on the P-wave morphology and the setting in which it occurs. Because each impulse originates in the sinoatrial node, the ECG shows a P wave preceding each QRS interval with a normal P-wave axis. In most cases, a secondary cause of sinus tachycardia can be identified. A careful assessment is important, to evaluate whether the sinus rate is appropriate for the clinical situation. Sinus tachycardia can be mistaken for other supraventricular arrhythmias, including atrial flutter, particularly with rapid tachyarrhythmias (when P waves are difficult to distinguish or when ectopic atrial foci originate near the sinoatrial node, such as near the superior vena cava or upper crista terminalis).
Atrial versus ventricular arrhythmia
Whether the arrhythmia originates from the atrium or the ventricle is usually dependent on whether the QRS complex is wide or narrow, and on the atrial:ventricular relationship. Atrial arrhythmias usually conduct to the ventricle through the His-Purkinje system and result in a narrow QRS complex. Some overlap may occur when conduction occurs with aberrancy (left or right bundle branch block), if there is pre-excitation, and in the presence of antiarrhythmic agents that may slow conduction (sodium channel blockers). If P waves are discernible, an atrial:ventricular relationship of <1 is highly suggestive of a ventricular origin, whereas a relationship >1 is highly suggestive of an atrial origin. A 1:1 atrial:ventricular relationship can occur with both atrial and ventricular arrhythmias.
Narrow versus wide QRS complex
Classification can also be based on whether there is a narrow- (QRS interval <120 ms) or wide- (QRS interval >120 ms) complex tachycardia. Narrow-QRS-complex tachycardia suggests that anterograde conduction and thus depolarization of the ventricle occurs through the atrioventricular (AV) node and His-Purkinje system. A wide-complex tachycardia suggests that conduction through the ventricle occurs through the slower myocyte-to-myocyte connections (because of either AV conduction via an accessory pathway or a ventricular origin) and can be seen even with sinus rhythm. However, atrial tachyarrhythmias that conduct aberrantly may present as a wide-complex tachycardia.[Figure caption and citation for the preceding image starts]: Sinus rhythm with preexcitationFrom the collection of Robert W. Rho, MD; used with permission [Citation ends].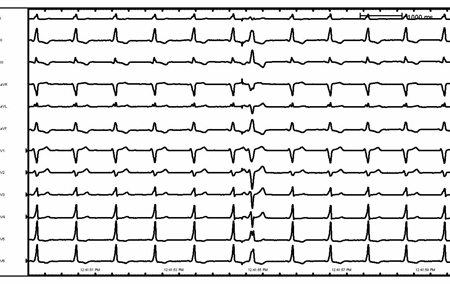 [Figure caption and citation for the preceding image starts]: Sinus rhythm with preexcitation (detail)From the collection of Robert W. Rho, MD; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Sinus rhythm with preexcitation (detail)From the collection of Robert W. Rho, MD; used with permission [Citation ends].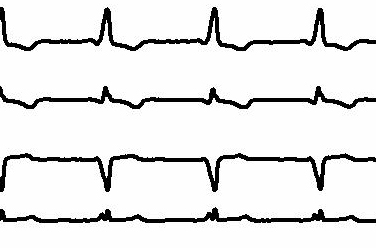
Regular versus irregular rhythm
Whether a rhythm is regular or irregular is easy to determine clinically and can help guide diagnosis of the tachyarrhythmia. An irregular rhythm is defined as a beat-to-beat R-R variability of more than 30 ms. In general, irregular narrow-complex arrhythmias include: atrial fibrillation, atrial flutter with variable conduction, and multifocal atrial tachycardia. An irregular wide-complex tachycardia may be due to pre-excited atrial fibrillation (due to a rapidly anterograde-conducting bypass tract), polymorphic ventricular tachycardia and atrial fibrillation, or multifocal atrial tachycardia conducting with aberrancy.
Site of origin
Tachyarrhythmias can be classified according to the site of origin: atrial, junctional, or ventricular:
Atrial impulses are characterized by initial depolarization of the atrium, from a single focus, such as sinus tachycardia or atrial tachycardia; macro reentry around an anatomic obstacle, such as in typical atrial flutter; or from multiple wavelets of reentry, such as atrial fibrillation.
Arrhythmias that originate at the level of the junction of the atrium and ventricle (AV node and/or proximal His bundle), such as AV nodal reentrant tachycardia or junctional ectopic tachycardia, are characterized by depolarization of the ventricle and retrograde atrial activation (if present), manifested by a retrograde P wave.
Arrhythmias that originate from the ventricle may originate from the distal His-Purkinje system or ventricular myocardium. The site of origin within the ventricle further defines some arrhythmias within the ventricle. Examples include right ventricular outflow tract ventricular tachycardia and bundle branch reentry ventricular tachycardia. Hemodynamic stability is not a helpful factor in differentiating atrial and ventricular arrhythmias. Some cases of ventricular tachycardia may be initially well tolerated hemodynamically. Misdiagnosis and inappropriate treatment (i.e., calcium channel blockers) may have catastrophic consequences.
When a patient with a wide-complex tachycardia is being evaluated and the diagnosis is not certain, the arrhythmia must be initially regarded as ventricular tachycardia until it is proved to be otherwise.
Epidemiology
Sinus tachycardia is the most common cause of sustained tachycardia, as it is usually a normal physiologic response to emotional or physical stimulation.[4]
Atrial fibrillation is the most common arrhythmia in clinical practice, with an estimated global prevalence of 52.55 million in 2021.[5][6] Up to 9% of patients aged 80 years or older have atrial fibrillation.[7][8] As the proportion of older people in the population increases, the number with atrial fibrillation is likely to increase significantly.
In the US, the prevalence of atrial fibrillation was estimated to be 10.55 million at the end of 2019.[6][9] In the European Union, prevalence of atrial fibrillation (in adults ages >55 years) is projected to increase from 8.8 million in 2010 to 17.9 million by 2060.[10]
The incidence of atrial flutter has been reported as 88 cases per 100,000 person-years; it is more common in men, with increasing age, and in those with heart failure or COPD.[11][12]
PSVT, defined as intermittent supraventricular tachycardia (AV node reentry tachycardia, AV reciprocating tachycardia, or atrial tachycardia) has an incidence of 57.8 cases per 100,000 person-years and a prevalence of 1.26 million people in the US.[13] Females are twice as likely to develop PSVT, and the incidence is five times greater in people older than 65 years compared with younger people.[14] Most cases of supraventricular tachycardia are due to AV nodal reentrant tachycardia (60% of cases); the remainder are due to AV reciprocating tachycardia (30%) and atrial tachycardia (10%).[15]
The prevalence of inappropriate sinus tachycardia is not well known and the underlying mechanisms are likely to be multifactorial, but patients are often young (age 15 to 50 years) and female.[1][2][16]
The prevalence of ventricular tachyarrhythmia is highly dependent on its type and duration. In patients with a history of previous MI, the incidence of sustained monomorphic ventricular tachyarrhythmia depends on the size of the infarction and the overall left ventricular function.
Differentials
Common
- Sinus tachycardia
- Acute atrial fibrillation
- Chronic atrial fibrillation
- Atrial flutter
- Atrial tachycardia
- AV nodal reentrant tachycardia
- AV reentry tachycardia/Wolff-Parkinson-White syndrome
- Multifocal atrial tachycardia
- Junctional ectopic tachycardia
- Monomorphic ventricular tachycardia with prior myocardial infarction
- Monomorphic ventricular tachycardia with nonischemic cardiomyopathy
- Ventricular fibrillation
- Polymorphic ventricular tachycardia with normal QT interval
- Idiopathic ventricular tachycardia: structurally normal heart
Uncommon
- Sinus node reentry tachycardia
- Inappropriate sinus tachycardia
- Permanent junctional reciprocating tachycardia
- Torsades de pointes
- Bidirectional ventricular tachycardia
- Accelerated idioventricular rhythm
- Postural orthostatic tachycardia syndrome
Contributors
Authors
Ramin Shadman, MD, FACC

Attending Physician
Southern California Permanente Medical Group
Assistant Professor of Medicine
UCLA
Los Angeles
CA
Disclosures
RS declares that he has no competing interests.
Robert W. Rho, MD, FACC

Attending Physician
Seattle
WA
Disclosures
RWR consults for Biosense Webster.
Peer reviewers
Attila Roka, MD, PhD
Cardiac Electrophysiologist
Creighton University
Omaha
NE
Disclosures
AR declares that he has no competing interests.
Mark M. Gallagher, BSc, MD
Consultant Cardiologist and Electro-physiologist
St George's Hospital
London
UK
Disclosures
MMG declares that he has no competing interests.
Fred Kusumoto, MD
Associate Professor of Medicine
Cardiovascular Diseases
Mayo Clinic
Jacksonville
FL
Disclosures
FK declares that he has no competing interests.
Zachary D. Goldberger, MD
Cardiology Fellow
University of Michigan Health System
Ann Arbor
MI
Disclosures
ZDG declares that he has no competing interests.
Peer reviewer acknowledgements
BMJ Best Practice topics are updated on a rolling basis in line with developments in evidence and guidance. The peer reviewers listed here have reviewed the content at least once during the history of the topic.
Disclosures
Peer reviewer affiliations and disclosures pertain to the time of the review.
References
Key articles
Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2016 Apr 5;67(13):e27-115.Full text Abstract
Katritsis DG, Boriani G, Cosio FG, et al. European Heart Rhythm Association (EHRA) consensus document on the management of supraventricular arrhythmias, endorsed by Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS), and Sociedad Latinoamericana de Estimulación Cardiaca y Electrofisiologia (SOLAECE). Europace. 2017 Mar 1;19(3):465-511.Full text Abstract
Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation. 2024 Jan 2;149(1):e1-156.Full text Abstract
Sheldon RS, Grubb BP 2nd, Olshansky B, et al. 2015 heart rhythm society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm. 2015 Jun;12(6):e41-63.Full text
Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2018 Sep 25;138(13):e272-391.Full text Abstract
Reference articles
A full list of sources referenced in this topic is available to users with access to all of BMJ Best Practice.
Use of this content is subject to our disclaimer