Summary
Definition
History and exam
Key diagnostic factors
- pain on defecation
- tearing sensation on passing stool
- fresh blood on stool or on paper
- anal spasm
Other diagnostic factors
- intermittent symptoms
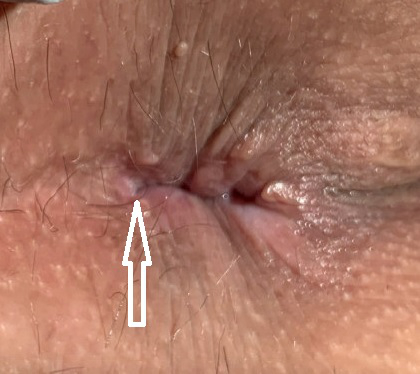
- sentinel pile
- fissure visible on retraction of buttock
Risk factors
- hard stool
- pregnancy
- opiate analgesia
Diagnostic tests
1st tests to order
- clinical diagnosis
Tests to consider
- anal manometry
- anal ultrasound
Treatment algorithm
on presentation
resistant fissures
Contributors
Authors
Nivedh Paluvoi, MD
Assistant Professor of Surgery
Colorectal Surgery
Miller School of Medicine
University of Miami
Coral Gables
FL
Disclosures
NP declares that he has no competing interests.
Acknowledgements
Dr Nivedh Paluvoi would like to gratefully acknowledge Dr John R. T. Monson, Dr John Scholefield, and Dr Jonathan Lund, previous contributors to this topic. JRTM declares that he has no competing interests. JS and JL are authors of a number of references cited in this topic.
Peer reviewers
Stephen H. Leveson, MD, FRCS
Professor
York Hospital
York
UK
Disclosures
SHL declares that he has no competing interests.
Steven Brown, MD, FRCS
Consultant Colorectal Surgeon
Northern General Hospital
Sheffield
UK
Disclosures
SB declares that he has no competing interests.
Jan Rakinic, MD, FACS, FASCRS
Associate Professor of Surgery
Chief
Section of Colorectal Surgery
Southern Illinois University School of Medicine
Springfield
IL
Disclosures
JR is an author of a reference cited in this topic.
Peer reviewer acknowledgements
BMJ Best Practice topics are updated on a rolling basis in line with developments in evidence and guidance. The peer reviewers listed here have reviewed the content at least once during the history of the topic.
Disclosures
Peer reviewer affiliations and disclosures pertain to the time of the review.
References
Key articles
Gilani A, Tierney G. Chronic anal fissure in adults. BMJ. 2022 Jan 12;376:e066834.
Lund JN, Nystrom PO, Coremans G, et al. An evidence-based treatment algorithm for anal fissure. Tech Coloproctol. 2006 Oct;10(3):177-80. Abstract
American Gastroenterological Association. American Gastroenterological Association medical position statement: diagnosis and care of patients with anal fissure. Gastroenterology. 2003 Jan;124(1):233-4.Full text
Davids JS, Hawkins AT, Bhama AR, et al. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the management of anal fissures. Dis Colon Rectum. 2023 Feb 1;66(2):190-9.Full text
Menteş BB, Irkörücü O, Akin M, et al. Comparison of botulinum toxin injection and lateral internal sphincterotomy for the treatment of chronic anal fissure. Dis Colon Rectum. 2003 Feb;46(2):232-7. Abstract
Reference articles
A full list of sources referenced in this topic is available to users with access to all of BMJ Best Practice.
Differentials
- Crohn disease
- Sarcoidosis
- Extrapulmonary Tuberculosis
More DifferentialsGuidelines
- Clinical practice guideline for the management of anal fissures
- Consensus guidelines in emergency colorectal surgery
More GuidelinesPatient information
Anal tears
More Patient information Log in or subscribe to access all of BMJ Best Practice
Log in or subscribe to access all of BMJ Best Practice
Use of this content is subject to our disclaimer