Summary
Definition
History and exam
Key diagnostic factors
- age 20-50 years
- female sex
- dyspnea
- accentuated pulmonic component (P2) to the second heart sound
- tricuspid regurgitation murmur
- family history
Other diagnostic factors
- fatigue
- peripheral edema
- cyanosis
- stimulant use
- syncope
- chest pain
- near syncope
- early diastolic, high-pitched murmur in the pulmonary area
- jugular vein distension
Risk factors
- family history
- female sex
- bone morphogenetic protein receptor type 2 (BMPR2) mutations
- appetite suppressants
- drugs and toxins
Diagnostic tests
1st tests to order
- chest radiography
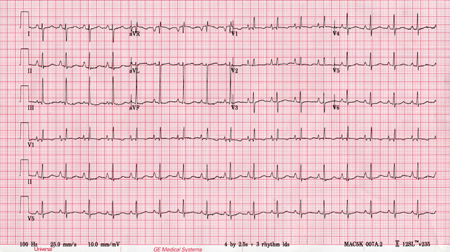
- ECG
- transthoracic Doppler echocardiography
- right heart catheterization
- antinuclear antibodies (ANA)
- pulmonary function tests
- arterial blood gas (ABG)
- nocturnal oximetry
- ventilation-perfusion (V/Q) scintigraphy
- 6-minute walk test
- B-type natriuretic peptide (BNP) or N-terminal proBNP (NT-proBNP)
- CBC
- LFTs
- thyroid function tests
- HIV serology
Tests to consider
- high-resolution chest CT scan ± CT pulmonary angiography
- cardiac MRI
- vasodilator testing with inhaled nitric oxide, inhaled iloprost, or intravenous epoprostenol
Treatment algorithm
positive response to acute vasoreactivity testing with no contraindication to calcium-channel blockers
negative response to acute vasoreactivity testing or contraindication to calcium-channel blockers: without cardiopulmonary comorbidity
negative response to acute vasoreactivity testing or contraindication to calcium-channel blockers: with cardiopulmonary comorbidity
Contributors
Authors
Muhammad Sameed, MD
Director Advance Lung Disease Program
Department of Pulmonary & Critical Care Medicine
Assistant Professor of Medicine
Thomas Jefferson University Hospital - Einstein Health
Philadelphia
PA
Disclosures
MS declares that he has no competing interests.
Gustavo A. Heresi, MD, MS

Director, Pulmonary Vascular and CTEPH Program
Department of Pulmonary and Critical Care Medicine
Respiratory Institute
Cleveland Clinic
Cleveland
OH
Disclosures
GAH has received speaking and advisory board fees from Bayer Healthcare, the manufacturer of riociguat.
Acknowledgements
Dr Muhammad Sameed and Dr Gustavo A. Heresi would like to gratefully acknowledge Dr Raed A. Dweik, a previous contributor to this topic.
Disclosures
RAD declares that he has no competing interests.
Peer reviewers
Michael J. Krowka, MD
Division of Pulmonary and Critical Care Medicine
Mayo Clinic College of Medicine
Rochester
MN
Disclosures
MJK declares that he has no competing interests.
Charlie Elliot, MB ChB, MRCP
Consultant Physician in Respiratory and General Internal Medicine
Sheffield Pulmonary Vascular Disease Unit
Royal Hallamshire Hospital
Sheffield
UK
Disclosures
CE has received reimbursement for attending several conferences as well as lecture fees from Actelion Pharmaceuticals, GSK, and Bayer.
Maria Giovanna Triveri, MD, PhD
Assistant Professor of Cardiology,
Medical Director of the Pulmonary Hypertension Program
Icahn School of Medicine at Mount Sinai Hospital
New York
NY
Disclosures
MGT has participated on Advisory Boards of Bayer and Actelion and received financial compensation for attendance.
Peer reviewer acknowledgements
BMJ Best Practice topics are updated on a rolling basis in line with developments in evidence and guidance. The peer reviewers listed here have reviewed the content at least once during the history of the topic.
Disclosures
Peer reviewer affiliations and disclosures pertain to the time of the review.
References
Key articles
Simonneau G, Montani D, Celermajer DS, et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J. 2019 Jan;53(1):1801913.Full text Abstract
Humbert M, Kovacs G, Hoeper MM, et al; ESC/ERS Scientific Document Group. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022 Oct 11;43(38):3618-731. [Erratum in: Eur Heart J. 2023 Feb 23:ehad005.]Full text Abstract
Rich S, Dantzker DR, Ayres SM, et al. Primary pulmonary hypertension. A national prospective study. Ann Intern Med. 1987 Aug;107(2):216-23. Abstract
Klinger JR, Elliott CG, Levine DJ, et al. Therapy for pulmonary arterial hypertension in adults: update of the CHEST guideline and expert panel report. Chest. 2019 Mar;155(3):565-86. [Erratum in: Chest. 2021 Jan;159(1):457.] Abstract
Frost A, Badesch D, Gibbs JSR, et al. Diagnosis of pulmonary hypertension. Eur Respir J. 2019 Jan;53(1):1801904.Full text Abstract
Galiè N, Channick RN, Frantz RP, et al. Risk stratification and medical therapy of pulmonary arterial hypertension. Eur Respir J. 2019 Jan;53(1):1801889.Full text Abstract
Reference articles
A full list of sources referenced in this topic is available to users with access to all of BMJ Best Practice.
Differentials
- Pulmonary arterial hypertension (PAH) associated with left-sided heart disease (pulmonary venous hypertension)
- PAH associated with respiratory diseases and/or hypoxia
- PAH due to chronic thrombotic and/or embolic disease
More DifferentialsGuidelines
- Pulmonary rehabilitation for adults with chronic respiratory disease
- 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension
More Guidelines Log in or subscribe to access all of BMJ Best Practice
Log in or subscribe to access all of BMJ Best Practice
Use of this content is subject to our disclaimer