Summary
Definition
Typical atrial flutter (counterclockwise cavotricuspid isthmus-dependent atrial flutter) is a macroreentrant atrial tachycardia with atrial rates usually above 250 bpm up to 320 bpm. It results from organized electrical activity in which large areas of the atrium take part in the reentrant circuit. The typical form depends on the so-called cavotricuspid isthmus for part of the circuit: the tricuspid annulus as the anterior boundary and the crista terminalis/eustachian ridge as the posterior boundary, as well as the endocardial cavity of the right atrium. The term counterclockwise refers to the direction of activation when the tricuspid annulus is viewed en face, whereby activation occurs up the septum, down the right atrial free wall in a counterclockwise fashion. Characteristic features on ECG are negatively directed saw-tooth atrial deflections (f waves) seen in leads II, III, and aVF, with positively directed deflections in lead V1.[1] This rhythm is closely related to atrial fibrillation.[2][3][4]
[Figure caption and citation for the preceding image starts]: Typical atrial flutter with variable (3 to 4:1) blockFrom the collection of Dr K.C. Wu [Citation ends]. [Figure caption and citation for the preceding image starts]: Atrial fibrillationFrom the collection of Dr K.C. Wu [Citation ends].
[Figure caption and citation for the preceding image starts]: Atrial fibrillationFrom the collection of Dr K.C. Wu [Citation ends].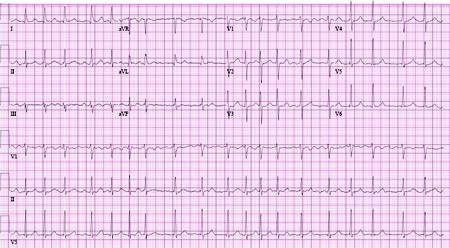 [Figure caption and citation for the preceding image starts]: Atrial flutter typically involves a circuit in the right atriumFrom: Cox D, Dougall H. Student BMJ. 2001;9:399-442; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Atrial flutter typically involves a circuit in the right atriumFrom: Cox D, Dougall H. Student BMJ. 2001;9:399-442; used with permission [Citation ends].
History and exam
Key diagnostic factors
- worsening heart failure or pulmonary symptoms
- jugular venous pulsations with rapid flutter waves
Other diagnostic factors
- palpitations
- fatigue or lightheadedness
- chest pain
- dyspnea
- syncope
- hypotension
- embolic events
Risk factors
- increasing age
- valvular dysfunction
- atrial septal defects
- atrial dilation
- recent cardiac or thoracic procedures
- surgical or postablation scarring of atria
- heart failure
- hyperthyroidism
- COPD
- asthma
- pneumonia
- antiarrhythmics for atrial fibrillation
- diabetes
- digitalis use
- male sex
- congenital or lone atrial flutter
Diagnostic tests
1st tests to order
- ECG
- thyroid function tests
- serum electrolytes
Tests to avoid
- imaging stress tests
- coronary CT angiography
Tests to consider
- pulmonary function tests
- CXR
- digitalis level
- cardiac enzymes
- spiral CT with pulmonary embolism protocol
- transthoracic echocardiogram
- atrial electrogram recording
- electrophysiologic studies
Treatment algorithm
hemodynamically unstable
hemodynamically stable
recurrent atrial flutter or failure of elective cardioversion
Contributors
Expert advisers
Komandoor Srivathsan, MD
Cardiac Electrophysiologist, Cardiologist
Mayo Clinic
Phoenix, AZ
Disclosures
KS declares that he has no competing interests.
Sai Anil Kumar Sriramoju, MD
Cardiovascular Disease Fellow
Garden City Hospital
Garden City, MI
Disclosures
SAKS declares that he has no competing interests.
Acknowledgement
BMJ Best Practice would like to gratefully acknowledge the previous expert contributor, whose work has been retained in parts of the content:
Katherine C. Wu MD, FACC
Associate Professor of Medicine
Johns Hopkins University
School of Medicine
Baltimore, MD
Disclosures
KCW declares that she has no competing interests.
Peer reviewers
Richard C. Wu, MD
Associate Professor of Medicine
Director
Cardiac Electrophysiology Laboratory
UT Southwestern Medical Center
University Hospital
St. Paul
Dallas, TX
Disclosures
RCW declares that he has no competing interests.
Reginald Ho, MD
Clinical Assistant Professor
Department of Medicine
Thomas Jefferson University Hospital
Philadelphia, PA
Disclosures
RH declares that he has no competing interests.
George Juang, MD, FACC
Director of Electrophysiology
Long Island Arrhythmia Center
Mineola, NY
Disclosures
GJ declares that he has no competing interests.
Peer reviewer acknowledgements
BMJ Best Practice topics are updated on a rolling basis in line with developments in evidence and guidance. The peer reviewers listed here have reviewed the content at least once during the history of the topic.
Disclosures
Peer reviewer affiliations and disclosures pertain to the time of the review.
References
Key articles
Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia. J Am Coll Cardiol. 2016 Apr 5;67(13):e27-115.Full text Abstract
Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation. 2024 Jan 2;149(1):e1-156.Full text Abstract
Van Gelder IC, Rienstra M, Bunting KV, et al. 2024 ESC guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2024 Sep 29;45(36):3314-414.Full text Abstract
Reference articles
A full list of sources referenced in this topic is available to users with access to all of BMJ Best Practice.
Differentials
- Atrial fibrillation
- Atrial tachycardia
More DifferentialsGuidelines
- 2024 ESC guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS)
- 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation
More GuidelinesCalculators
Atrial Fibrillation CHA(2)DS(2)-VASc Score for Stroke Risk
HAS-BLED Bleeding Risk Score
More CalculatorsVideos
Electrical (direct current) cardioversion animated demonstration
More videosPatient information
Atrial fibrillation: what is it?
Atrial fibrillation: what are the treatment options?
More Patient information Log in or subscribe to access all of BMJ Best Practice
Log in or subscribe to access all of BMJ Best Practice
Use of this content is subject to our disclaimer