Summary
Definition
Barrett esophagus is a change in the normal squamous epithelium of the esophagus to specialized intestinal metaplasia.[1] This is associated with gastroesophageal reflux, even if the reflux is asymptomatic.[2][3] Essential to the diagnosis is histology demonstrating columnar-lined epithelium, with or without intestinal metaplasia and with goblet cells.[4] Beyond gastroesophageal reflux-related symptoms, the main concern is the increased risk of adenocarcinoma of the esophagus.[2][3][Figure caption and citation for the preceding image starts]: Barrett esophagus; note salmon-colored mucosa extending superior to the gastroesophageal junction as a continuous columnFrom the personal collection of Dr Vic Velanovich; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Barrett esophagus; note salmon-colored mucosa extending superior to the gastroesophageal junction with marked irregular borderFrom the personal collection of Dr Vic Velanovich; used with permission [Citation ends].
[Figure caption and citation for the preceding image starts]: Barrett esophagus; note salmon-colored mucosa extending superior to the gastroesophageal junction with marked irregular borderFrom the personal collection of Dr Vic Velanovich; used with permission [Citation ends]. [Figure caption and citation for the preceding image starts]: Barrett metaplasia without dysplasia, demonstrating columnar epithelium with goblet cells from superior to the gastroesophageal junctionCourtesy of Adrian Ormsby, MD, Henry Ford Hospital, Detroit, MI [Citation ends].
[Figure caption and citation for the preceding image starts]: Barrett metaplasia without dysplasia, demonstrating columnar epithelium with goblet cells from superior to the gastroesophageal junctionCourtesy of Adrian Ormsby, MD, Henry Ford Hospital, Detroit, MI [Citation ends].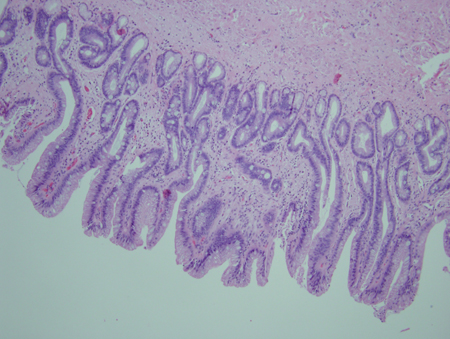 [Figure caption and citation for the preceding image starts]: Barrett metaplasia with low-grade dysplasia; note the more irregular cells and nucleiCourtesy of Adrian Ormsby, MD, Henry Ford Hospital, Detroit, MI [Citation ends].
[Figure caption and citation for the preceding image starts]: Barrett metaplasia with low-grade dysplasia; note the more irregular cells and nucleiCourtesy of Adrian Ormsby, MD, Henry Ford Hospital, Detroit, MI [Citation ends].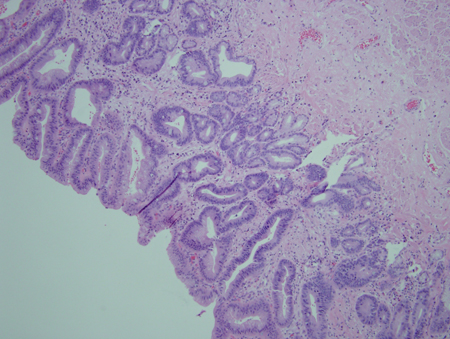 [Figure caption and citation for the preceding image starts]: Barrett metaplasia with high-grade dysplasia; note more advanced irregularity of the cellsCourtesy of Adrian Ormsby, MD, Henry Ford Hospital, Detroit, MI [Citation ends].
[Figure caption and citation for the preceding image starts]: Barrett metaplasia with high-grade dysplasia; note more advanced irregularity of the cellsCourtesy of Adrian Ormsby, MD, Henry Ford Hospital, Detroit, MI [Citation ends]. [Figure caption and citation for the preceding image starts]: Barrett metaplasia with high-grade dysplasia associated with a focus of intramucosal carcinoma; note the frankly malignant cells beyond the confines of the basement membrane to involve the lamina propriaCourtesy of Adrian Ormsby, MD, Henry Ford Hospital, Detroit, MI [Citation ends].
[Figure caption and citation for the preceding image starts]: Barrett metaplasia with high-grade dysplasia associated with a focus of intramucosal carcinoma; note the frankly malignant cells beyond the confines of the basement membrane to involve the lamina propriaCourtesy of Adrian Ormsby, MD, Henry Ford Hospital, Detroit, MI [Citation ends].
History and exam
Key diagnostic factors
- heartburn
- regurgitation
- dysphagia
Other diagnostic factors
- incidental finding during gastrointestinal endoscopy for other indication
- chest pain
- laryngitis
- cough
- dyspnea or wheezing
- history of aspiration pneumonia
Risk factors
- acid/bile reflux or GERD
- increased age
- white ethnicity
- male sex
- family history of Barrett esophagus or esophageal adenocarcinoma
- obesity
- smoking
Diagnostic tests
1st tests to order
- upper GI endoscopy with biopsy
- barium esophagogram
Emerging tests
- chromoendoscopy
- autofluorescence imaging
- confocal laser endomicroscopy
- optical coherence tomography
- spectroscopy
- transnasal endoscopy
- capsule endoscopy
- gelatin-coated sponge
Treatment algorithm
nondysplastic Barrett esophagus
low-grade dysplasia
high-grade dysplasia
Contributors
Authors
Andres F. Carrion, MD
Associate Professor of Medicine
Division of Gastroenterology and Hepatology
University of Miami
Miller School of Medicine
Miami
FL
Disclosures
AFC is a scientific advisor for Intercept Pharmaceuticals and Gilead Sciences, and is on the speaker bureau for Bristol-Myers Squibb, Intercept Pharmaceuticals, Merck, and Alexion.
Ricardo Badillo, MD
Assistant Professor of Medicine
Division of Gastroenterology
Texas Tech University Health Sciences Center
El Paso
TX
Disclosures
RB declares that he has no competing interests.
Marc J. Zuckerman, MD
Professor of Medicine
Chief
Division of Gastroenterology
Texas Tech University Health Sciences Center
El Paso
TX
Disclosures
MJZ is on the speakers bureau for Phathom Pharmaceuticals.
Acknowledgements
Dr Andres F. Carrion, Dr Ricardo Badillo and Dr Marc J. Zuckerman would like to gratefully acknowledge Dr Vic Velanovich, the previous contributor to this topic.
Disclosures
VV is an author of a number of references cited in this topic.
Peer reviewers
Richard E. Sampliner, MD
Professor
Medicine Chief
Department of Gastroenterology
University of Arizona College of Medicine
Tucson
AZ
Disclosures
RES declares that he has no competing interests.
Peter McCulloch, MBChB, MA, MD, FRCS (Ed), FRCS (Glas)
Clinical Reader in Surgery
Nuffield Department of Surgery
University of Oxford
Oxford
UK
Disclosures
PM declares that he has no competing interests.
Peer reviewer acknowledgements
BMJ Best Practice topics are updated on a rolling basis in line with developments in evidence and guidance. The peer reviewers listed here have reviewed the content at least once during the history of the topic.
Disclosures
Peer reviewer affiliations and disclosures pertain to the time of the review.
References
Key articles
Fitzgerald RC, di Pietro M, Ragunath K, et al. British Society of Gastroenterology guidelines on the diagnosis and management of Barrett's oesophagus. Gut. 2014 Jan;63(1):7-42.Full text Abstract
Shaheen NJ, Falk GW, Iyer PG, et al. Diagnosis and management of Barrett's esophagus: an updated ACG guideline. Am J Gastroenterol. 2022 Apr 1;117(4):559-87.Full text Abstract
Fitzgerald RC. Molecular basis of Barrett's oesophagus and oesophageal adenocarcinoma. Gut. 2006 Dec;55(12):1810-20. Abstract
Weusten B, Bisschops R, Coron E, et al. Endoscopic management of Barrett's esophagus: European Society of Gastrointestinal Endoscopy (ESGE) position statement. Endoscopy. 2017 Feb;49(2):191-8.Full text Abstract
Sharma P, Dent J, Armstrong D, et al. The development and validation of an endoscopic grading system for Barrett's esophagus: the Prague C & M criteria. Gastroenterology. 2006 Nov;131(5):1392-9.Full text Abstract
Reference articles
A full list of sources referenced in this topic is available to users with access to all of BMJ Best Practice.
Differentials
- Esophagitis
- GERD
- Esophageal adenocarcinoma
More DifferentialsGuidelines
- Endoscopic eradication therapy of Barrett’s esophagus and related neoplasia
- Adverse events associated with EGD and EGD-related techniques
More GuidelinesPatient information
Acid reflux, heartburn, and gastroesophageal reflux disease (GERD)
More Patient information Log in or subscribe to access all of BMJ Best Practice
Log in or subscribe to access all of BMJ Best Practice
Use of this content is subject to our disclaimer