Summary
Definition
History and exam
Key diagnostic factors
- recurrent episodes of binge eating
- recurrent inappropriate compensatory behavior
- eating disturbance not exclusively during periods of anorexia nervosa
- depression and low self-esteem
- concern about weight and body shape
- dental erosion
- parotid hypertrophy
- Russell sign
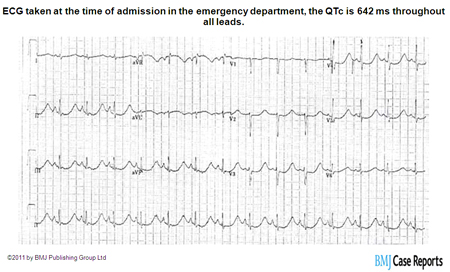
- arrhythmia
Other diagnostic factors
- age 20-35 years
- menstrual irregularity
- drug-seeking behavior
- deliberate misuse of insulin
- self-injurious behavior
- gastrointestinal symptoms
- history of dieting
- marked fluctuations in weight
- shoplifting behavior
- use of ipecac
- needle marks on skin
- vomiting in pregnancy
Risk factors
- female sex
- personality disorder
- body image dissatisfaction
- history of sexual abuse
- impulsivity
- family history of alcoholism
- family history of depression
- family history of eating disorder
- childhood overweight or obesity
- exposure to media pressure
- early onset of puberty
- urbanization
- family history of obesity
- participation in elite-level sports
Diagnostic tests
1st tests to order
- serum electrolytes
- serum creatinine
- serum magnesium
- urine pregnancy test
- serum LFTs
- serum creatine kinase (CK)
- CBC
- urinalysis
Tests to consider
- ECG
- serum ferritin
- serum B12
- serum red blood cell folate
- dual-energy x-ray absorptiometry scan for bone density
Treatment algorithm
nonpregnant adults
children and adolescents
pregnant
Contributors
Authors
Debra L. Safer, MD
Associate Professor
Co-Director of Stanford Eating and Weight Disorders Program
Stanford University School of Medicine
Department of Psychiatry & Behavioral Sciences
Stanford
CA
Disclosures
DLS is an author of a reference cited in this topic, and receives royalties from Guilford Press for books on adapting dialectical behavior therapy for eating disorders.
Acknowledgements
Dr Debra L. Safer would like to gratefully acknowledge Dr David C.W. Lau and Dr C. Laird Birmingham, the previous contributors to this topic.
Disclosures
DCWL declares that he has no competing interests. CLB is an author of several references cited in this topic.
Peer reviewers
Mimi Israel, MD, FRCPC
Chair of Psychiatry
McGill University
Quebec
Canada
Disclosures
MI declares that she has no competing interests.
Joel Yager, MD
Professor
Department of Psychiatry
University of New Mexico School of Medicine
Albuquerque
NM
Disclosures
JY is an author of a reference cited in this topic.
Peer reviewer acknowledgements
BMJ Best Practice topics are updated on a rolling basis in line with developments in evidence and guidance. The peer reviewers listed here have reviewed the content at least once during the history of the topic.
Disclosures
Peer reviewer affiliations and disclosures pertain to the time of the review.
References
Key articles
American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 5th ed., text revision (DSM-5-TR). Washington, DC: American Psychiatric Publishing; 2022.
Academy for Eating Disorders. Eating disorders: critical points for early recognition and medical risk management in the care of individuals with eating disorders. 2021 [internet publication].Full text
Lock J, La Via MC, American Academy of Child and Adolescent Psychiatry (AACAP) Committee on Quality Issues (CQI). Practice parameter for the assessment and treatment of children and adolescents with eating disorders. J Am Acad Child Adolesc Psychiatry. 2015 May;54(5):412-25.Full text Abstract
Carl RL, Johnson MD, Martin TJ; Council on Sports Medicine and Fitness. Promotion of healthy weight-control practices in young athletes. Pediatrics. 2017 Sep;140(3): e20171871.Full text Abstract
Morgan JF, Reid F, Lacey JH. The SCOFF questionnaire: assessment of a new screening tool for eating disorders. BMJ. 1999 Dec 4;319(7223):1467-8.Full text Abstract
National Institute for Health and Care Excellence (UK). Eating disorders: recognition and treatment. 16 December 2020 [internet publication].Full text
Reference articles
A full list of sources referenced in this topic is available to users with access to all of BMJ Best Practice.
Differentials
- Other specified feeding or eating disorder (OSFED), or unspecified feeding or eating disorder (UFED)
- Anorexia nervosa, binge-eating/purging subtype
- Binge-eating disorder
More DifferentialsGuidelines
- The hospitalized adolescent
- Practice guideline for the treatment of patients with eating disorders
More GuidelinesPatient information
Bulimia: what is it?
Bulimia: what are the treatment options?
More Patient information Log in or subscribe to access all of BMJ Best Practice
Log in or subscribe to access all of BMJ Best Practice
Use of this content is subject to our disclaimer